






Introduction
Abortion is the termination of pregnancy by the removal or expulsion of a fetus or embryo from the uterus, prior to viability. An abortion that occurs spontaneously is usually called a miscarriage. Most spontaneous embryonic abortions occur during the first 3 weeks [1]. It is generally thought that 15–20% of verified pregnancies that have survived the first 4 weeks post-ovulation are lost through spontaneous abortion. A high incidence of spontaneous abortion of fetuses with neural tube defects, cleft lip, and cleft palate has been noted among malformed embryos, and many other external malformations may be involved in abortions [1,2]. However, the cause of abortion of normal conceptuses remains unknown, mainly due to the following issues: the difficulty in obtaining appropriate sample materials, and the small size of the embryos that makes analyses to find the internal abnormality difficult. The crown-rump length of an embryo is a maximum of 30 mm during the embryonic period by Carnegie stage (CS) 23 (about 56-60 days after fertilization) [3].
In the present report, two cases of liver agenesis were detected using phase-contrast X-ray computed tomography (PCT), and described in detail [4]. This novel abnormality could seriously disrupt embryonic development, and, as a result, may have led to early miscarriage. The causes of intrauterine death in externally normal embryos have not previously been elucidated, and the present report is a first step in that direction.
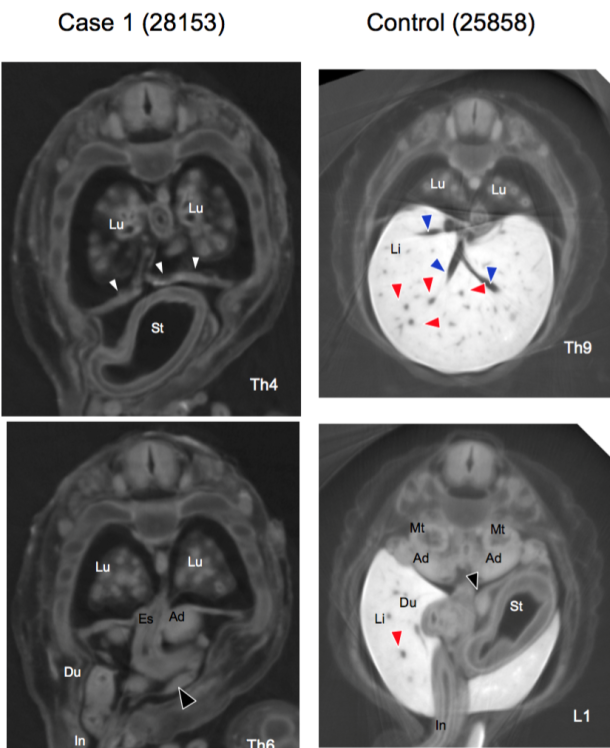
No liver (Li) was detected in the serial plane sections, while the stomach (St) was observed in the midsagittal transverse sections at Th4. The diaphragm (△) was noted in these sections. The duodenum (Du) was located on the right ventral side of the abdomen, while the pancreas (▼) had deviated to the ventral side in the Th6 transverse section. Umbilical vein and ductus venosus was not shown in this Figure.
Lung (Lu), esophagus (Es), adrenal gland (Ad), intestine (In), metanephros (Mt), liver (Li), portal veins (▲), and hepatic veins (▲).
Material and Methods
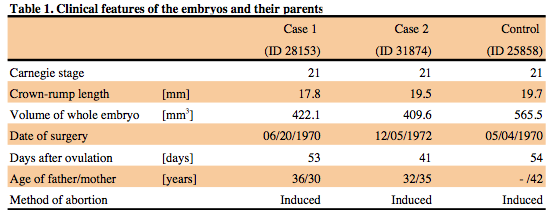
Images of three embryos at CS 21 were acquired using PCT imaging. The embryos werecollected and stored at the Congenital Anomaly Research Center of Kyoto University [5]. All three embryos were obtained by induced abortion (Table 1). The sizes and gestational ages were within the normal range. No clinical finding that may have caused an abnormality (i.e. alcohol, tobacco, drugs, etc) was observed. Obvious damage to, or anomalies of the external forms were not present. The embryo body axes were maintained in the original form, i.e. not artificially deformed during fixation and preservation. Therefore, the samples were judged to be suitable for internal structural analysis. The three-dimensional (3-D) PCT images of the human embryos were acquired using a radiographic imaging system (BL14-C, 17.8 Kev) from Photon Factory, Institute of Materials Structure Science, High Energy Accelerator Research Organization (KEK, Tsukuba, Japan). The data provide a resolution of ≥ 18 µm/pixel. This technique enables a highly sensitive measurement, approximately > 1000 times more sensitive than the conventional radiographic method using absorption contrast. The mechanism and conditions used to acquire the PCT images of the embryos have been described elsewhere [4]. The 3-D images included images of the intrathoracic, retroperitoneal, and intra-abdominal organs, reconstructed using Amira software (ver. 5.4.5, Visage Imaging, Berlin, Germany).
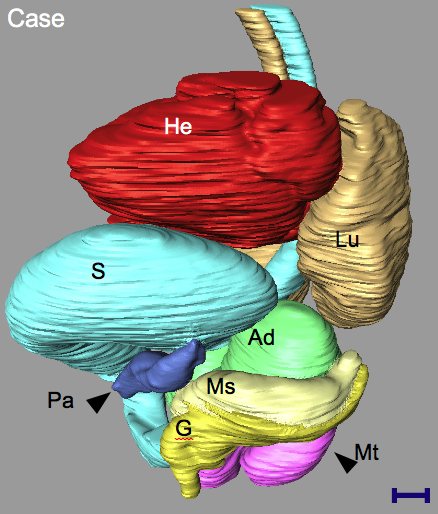
Left anterior oblique view of the three-dimensional PCT reconstruction of Case 1, demonstrating the locations of all intra-thoracic, retroperitoneal, and intraabdominal organs.
The findings of note were as follows: agenesis of the liver; the stomach (St) was deviated ventrally and cranially; the pancreas (Pa) was deviated ventrally; and the right mesonephros (Ms) and genital ridge (Ge) were absent.
Lung (Lu), adrenal gland (Ad), metanephros (Mt), and heart (He).
The scale bar in the reconstructed image indicates 1 mm.
Results and discussion
The liver at CS21 usually occupies a large space in the abdominal cavity, which has a smooth surface due to the contact between the cranial surface and the diaphragm, and between the ventral surface and the abdominal wall [6]. The PCT image resolution was high enough to observe not only the morphological structure of the internal organs but also the internal structure of the liver.
A PCT plane section showed the main structures of the vascular systems, such as the umbilical vein, ductus venosus, hepatic veins, portal vein, and their branches, in a control case (Figure 1). In the two abnormal cases, the liver was not detected in any of the serial plane sections. In Case 1 (ID 28153), the stomach was observed on the midsagittal line in the Th4 transverse sections, indicating that the stomach had deviated cranially and ventrally. The diaphragm was apparent in these sections. The duodenum was located in the right ventral part of the abdomen, and the pancreas deviated ventrally in the Th6 transverse section. Similar abnormalities were detected in Case 2 (ID 31874), which also had no detectable liver (data not shown).
The locations of all intrathoracic, retroperitoneal, and intra-abdominal organs were reconstructed in three dimensions, as shown in Figure 2. The liver, which usually occupied a large space, was not detectable at all. The right genital ridge and mesonephros were not present.
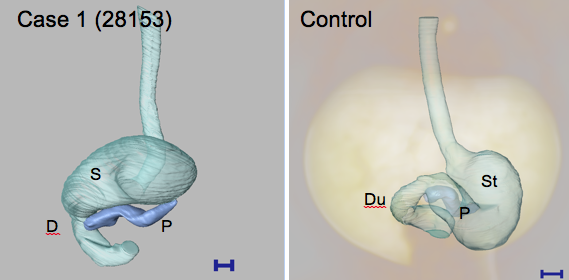
The absence of the liver in Case 1 had affected the locations of the other internal organs, especially the stomach, duodenum, and pancreas (Figure 3). The stomach was rotated. The pyloric antrum was straight, and ran vertically in the right ventral quadrant. Notably, the relative positions of the cardia and pylorus were not affected. The pancreas originated from the duodenum, and its tail had deviated ventrally. Similar complications were detected in Case 2 (data not shown).
The liver plays an important role in the development of functional organs [6,7]. The liver becomes a hematopoietic organ after 6 weeks, and, during the fetal period, begins to metabolize biochemical materials important for development, such as albumin, bile, glycogen, and fetus-specific proteins [8]. Therefore, liver agenesis may be lethal to development.
The present study demonstrates that PCT may be considered a powerful tool for visualization of internal structures of embryos, and for detection of novel abnormalities during the embryonic period, without the need for histological analysis. The non-invasive and non-destructive properties of the technique are important for analysis of scarce specimens, such as human embryos. The application of the present method will contribute to advancing the field of fetal diagnosis and developmental anatomy.
References
1. O’rahilly R, Müller F. Human embryology & teratology. 92 (2001)
2. Shiota K. Congenital Anomalies, 31, 67 (1991)
3. O’Rahilly R, Müller F. Developmental stages in human embryos: including a revision of Streeter’s” horizons” and a survey of the Carnegie Collection, (1987)
4. Yoneyama A, Yamada S, Takeda T. Advanced Biomedical Engineering, 107(2011)
5. Nishimura H, et al. Teratology, 1,281(1968)
6. Hirose A, et al. Anat Rec, 295, 51(2012)
7. Lemaigre FP. Gastroenterology, 137, 62(2009)
8. Tavian M, Hallais M, Péault B. Development, 126, 793(1999)