Details of the bronchial tree formation remain unknown because of the difficulty in analyzing extremely small embryos. We aimed to elucidate the morphogenesis of the human embryonic bronchial tree using phase-contrast X-ray computed tomography (PXCT) images. The three-dimensional (3D) branching of the bronchial trees was reconstructed using PXCT images in a sample of embryos (between n. The images revealed that branching variants arose during the embryonic period and continued throughout life. All proximal bronchi, except the were formed by a monopodial branching mode. The 3D reconstructions of the embryonic bronchial trees provided novel insights into how bronchial trees are generated in the small embryos.
The bronchial tree of the human lung is composed of conducting and respiratory airways [1]. This organ has a highly ramified structure in the lungs. An understanding of branching morphogenesis is essential for the diagnosis and treatment of congenital anomalies. However, how such complicated branching networks are generated during development remains unclear because of the difficulty in analyzing extremely small embryos. Recently, we provided new insights into the branching tree formation in the human embryonic lung by analyzing 3D reconstructions of the human embryonic bronchial tree [2, 3].
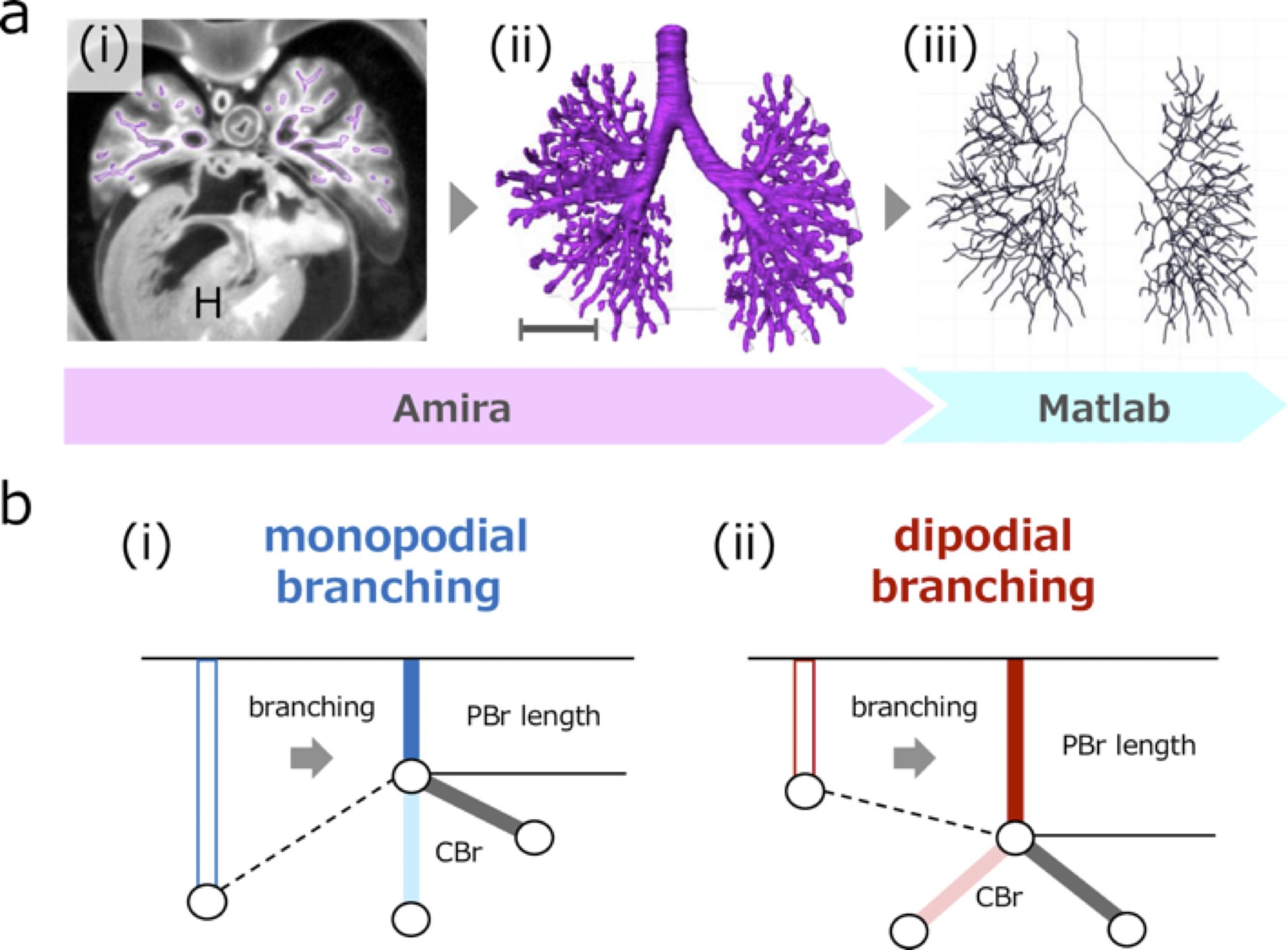
Figure 1: Image processing of the bronchial tree and illustration showing the change of bronchus length with monopodial and dipodial branching. a (i) Transverse section using phase-contrast X-ray computed tomography. Heart (H). (ii) Reconstructed bronchial tree. Scale bar: 1mm. (iii) Centerline was calculated based on reconstruction. b The parent bronchus (PBr) length may shrink with monopodial branching just after generation of child bronchus (CBr) (i), but may not shrink or elongate with dipodial branching (ii).
First, we extended the morphological analysis to the end of the embryonic period [2]. The embryonic period is from the time of fertilization to 8 weeks post-fertilization. It begins with the formation of the body structures, generally described by a standardized system of 23 stages called the Carnegie stages (CS) [4]. Previous morphological studies have demonstrated the general morphogenetic processes of the human bronchial tree during the embryonic period. The primordium of the tree buds extends from the middle of the foregut at approximately CS 12 (at approximately 4 weeks after fertilization) [5]. After that, this pulmonary primordium bud continues to extend and branches out continuously to form the lobar, segmental, and more peripheral branches. The first generation of sub-segmental bronchi is complete at CS19 [6]. However, morphological changes in the trees after CS20 have not been elucidated.
Second, we analyzed how the proximal bronchus of the human lung branched off [3]. Previous studies have proposed two simple branching modes: monopodial and dipodial [7, 8]. With monopodial branching, the child branches extend from the sidewall of the parent branch. With dipodial branching, the tip of the bronchus bifurcates. Previous studies estimated the branching mode based only on visual assessments.
Thus, we aimed to describe the morphogenesis of bronchial trees during the human embryonic period. We reconstructed 3D branching trees using phase-contrast X-ray computed tomography (PXCT) images, observed the morphological changes in the trees in detail, and categorized the branching mode as monopodial and dipodial based on the bronchus length.
A total of 48 embryos between CS15 and CS23 (about 5-8 weeks after fertilization, 8-30 mm crown-rump length) [4] of the Kyoto Collection were selected [9]. Imaging data of all samples were acquired using PXCT. The system was set up at the vertical wiggler beamline (BL-14C). The PXCT imaging data provided a resolution of ≥ 18 μm/pixel [10], which enabled the non-destructive observation of intrabody structures in detail, and the highly sensitive morphometry of the embryos. The structure of the bronchial tree was reconstructed for all samples using Amira software (version 6.2.0; Visage Imaging GmbH, Berlin, Germany) (Fig. 1a). The center of the airway was observed linearly with the centerline module. The coordinates were analyzed using MATLAB v. R2018a (MathWorks, Inc., Natick, MA, USA) to calculate the generation of all branches and branch lengths.
We categorized the branching modes of the lobar, segmental, and subsegmental bronchi. After calculating each bronchus length, we categorized the branching mode of the analyzed bronchi based on whether the parent bronchus was divided after generating the analyzed bronchi (Fig.1b).
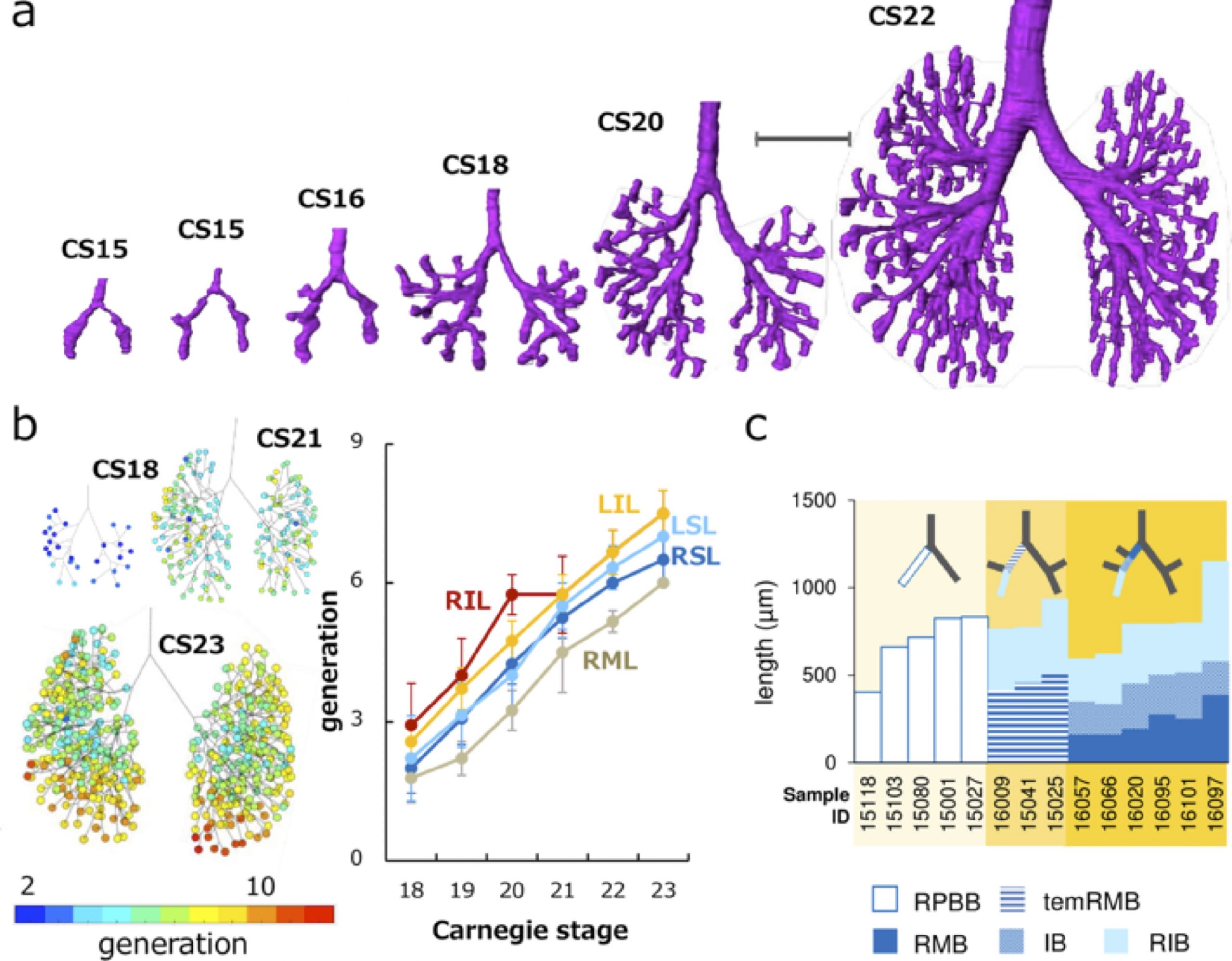
Figure 2: 3D reconstructions enable novel analyses of the human embryonic bronchial tree. a Representative reconstructions of the bronchial tree. Scale bar: 1mm. b (left) Generation of end-branching (rainbow color) at CS18, CS21, and CS23. The colored circle indicates generations of each end-branch when the lobar bronchus was defined as 0th branch. Color bar indicates the corresponding colors. (right) Change of generation in each lobe by Carnegie stage during CS18 and CS23. LIL, left inferior lobe; LSL, left superior lobe; RIL, right inferior lobe; RML, right middle lobe; RSL, right superior lobe. c Branching mode of the right superior and middle lobar bronchi. The length changes of the right proximal bronchi are shown. Compared with the right primary bronchial bud (RPBB) length before branching, temRMB length and total length of right main bronchus (RMB) and intermediate bronchus (IB) were shorter. RIB, right inferior bronchus; temRMB, temporary RMB branch from the tracheal bifurcation to the base of the right middle lobe.
Three-dimensionally reconstructed bronchial trees revealed a timeline of morphogenesis during the embryonic period (Fig. 2a). The right superior lobar bronchus was formed after the generation of both the right middle and left superior lobar bronchi. The distribution of the end-branch generation among the five lobes was significantly different (Fig. 2b). The median branching generation value in the right middle lobe was significantly lower than that in the other four lobes. Variations found between CS20 and CS23 were all described in the human adult lung, indicating that variation in the bronchial tree may arise during the embryonic period and continue throughout life.
All lobar bronchi were formed with monopodial branching (Fig. 2c). Twenty-five bifurcations were analyzed to categorize the branching mode of the segmental and subsegmental bronchi. Of these, 22 bifurcations were categorized as monopodial branching, two bifurcations were not categorized as any branching pattern, and the only lingular bronchus that bifurcated from the left superior lobar bronchus was categorized as dipodial branching.
High-resolution imaging data of human embryonic specimens using PXCT enabled the reconstruction of the three-dimensional bronchial tree, revealing morphogenetic changes during the human embryonic period. Our novel understanding of bronchial tree development will provide a crucial resource for elucidating congenital anomalies.
Fujii, T. Takakuwa (Kyoto Univ.)
REFERENCES
Standring, S, Gray’s Anatomy (Elsevier. 2015)
Fujii, T. Muranaka, J. Matsubayashi, S. Yamada, A. Yoneyama and T. Takakuwa, J. Anat.237 (2020).
Fujii, T. Muranaka, J. Matsubayashi, S. Yamada, A. Yoneyama and T. Takakuwa, PLoS ONE16, 1 (2021)
O’Rahilly and F. Müller, Developmental stages in human embryos: including a revision of Streeter’s” horizons” and a survey of the Carnegie Collection, (Carnegie Institution of Washington Publishing. 1987).
Streeter, G.L., Contributions to Embryology Carnegie Institution of Washington, 31 (1945)
Wells, L. and Boyden, E. American Journal of Anatomy, 95 (1954)
Palmer, D. M. Ohio Journal of Science, 36 (1936).
Metzger RJ, Klein OD, Martin GR and Krasnow MA, Nature. 453, 7196 (2008).
Nishimura, K. Takano, T. Tanimura and M. Yasuda, Teratology, 1 (1968).
Yoneyama, S. Yamada and T. Takeda, “Fine Biomedical Imaging Using X-Ray Phase-Sensitive Technique” in Advanced Biomedical Engineering, edited by G. D. Gargiulo and A. McEwan, 107-128. InTech Publishinng 2011.
The cause of spontaneous abortion of normal conceptuses remains unknown in most embryos because of the difficulty of diagnosing too small embryos. We aimed to reveal latent liver abnormalities using novel phasecontrast radiographic computed tomography (PXCT). Embryos with liver volumes ≥ 2 SD above or below the mean for the stage of development were screened from 1156 MR images from the Kyoto Collection. Selected embryos were further analyzed by using PXCT. Liver abnormality was detected in 9 embryos by our protocol. Most of such liver abnormality embryos do not survive, as liver function becomes essential.
The cause of spontaneous abortion of normal conceptuses remains unknown in most embryos [1] because of the difficulty of obtaining appropriate embryo materials as well as diagnosing internal abnormalities in very small embryos. The crown-rump length of an embryo is ranging 23 to 32 mm during the embryonic period by Carnegie stage (CS) 23 (about 56–60 days after fertilization) [2], by which stage all primordia of the organs are already provided.
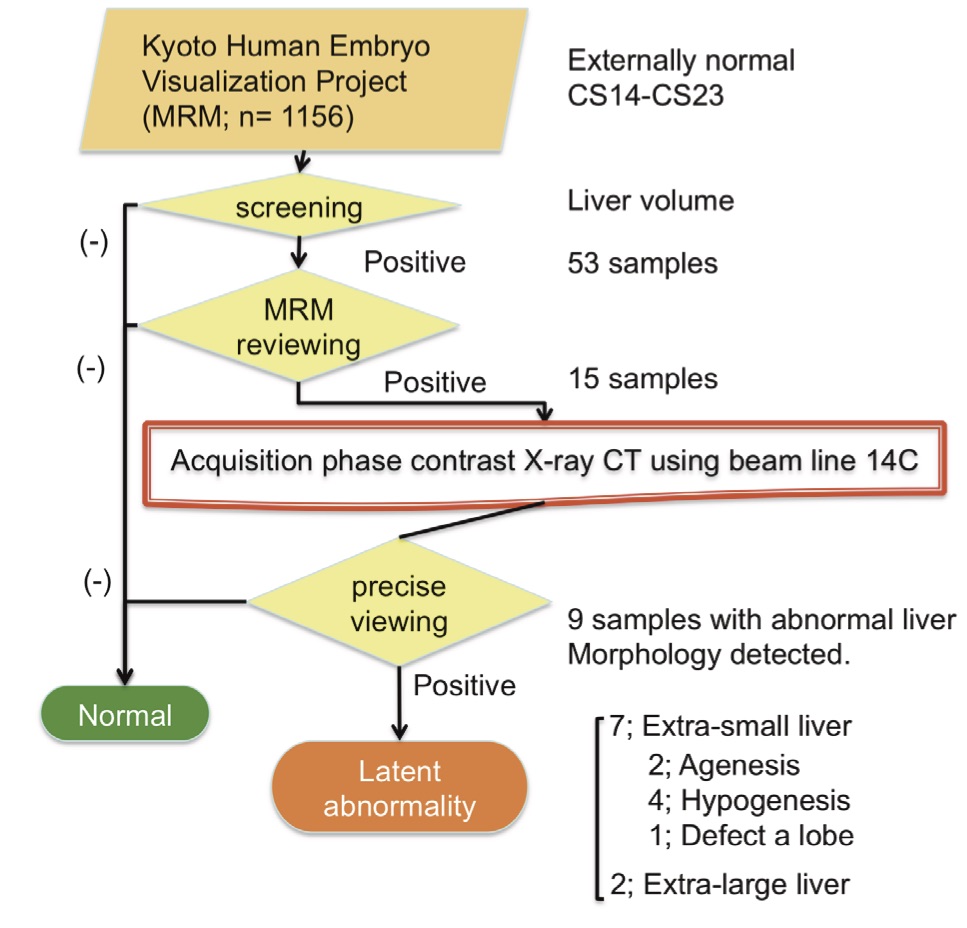
Figure 1: Protocol for detecting latent abnormal embryos that may result in spontaneous abortion.
Many factors are involved in spontaneous abortion, not only the embryonic factor itself but also maternal health and the intrauterine environment affected by unspecified modulators. Such complicated factors distract attention from the laborious inspection of embryos, especially when embryos are externally normal.
More than 40,000 embryo and fetal specimens have been collected in the Kyoto Collection since 1961 for revealing the mechanism of congenital anomalies [3]. An MRI database of approximately 1200 well-preserved human embryos, diagnosed as externally normal, was acquired in 2000–2005 (the Kyoto embryo visualizing project) [4] to observe a number of normal human embryos. The database has proven to be useful for research purposes and as a teaching material [5].
Although the MRI database includes only externally normal embryo specimens, whether the internal organs were also normal cannot be guaranteed. Considering that the cumulative intrauterine mortality rate in normal conceptuses was estimated at 18% [1], the MRI database includes embryos that have potential abnormalities that would have led to spontaneous abortion. Thus, detailed observation of the internal organs of embryo specimens from the database may provide clues to spontaneous abortion in the embryonic and fetal periods. In this connection, we aimed to determine the latent abnormalities that may cause spontaneous abortion by using the MRI database and novel phase-contrast radiographic computed tomography (PXCT).
The MRI database was screened by using the volume of the liver as the target organ. Embryos with liver
volumes ≥ 2 SD above or below the mean for the stage of development were selected. Embryos with potentially abnormal livers were further analyzed by using PXCT. The PXCT data provide a resolution of ≥ 18 μm/pixel, which enabled highly sensitive measurement, approximately > 1000 times more sensitive than the conventional radiographic method using absorption contrast [6].
Liver abnormality was detected in 9 embryos after the procedure of our protocol (Fig. 1), which consisted of hepatic agenesis (2 embryos), hepatic hypogenesis (4), liver lobe defect (1), involvement of the liver to the thoracic cavity by diaphragm herniation (1), and other (1). Three embryos had only liver abnormalities and 6 exhibited complications in other organs. The prevalence of liver malformations in CS18 and CS21 in the intrauterine population of externally normal embryos is approximately 1.7%. Most of such liver abnormality embryos do not survive, as liver function becomes essential during development [7].
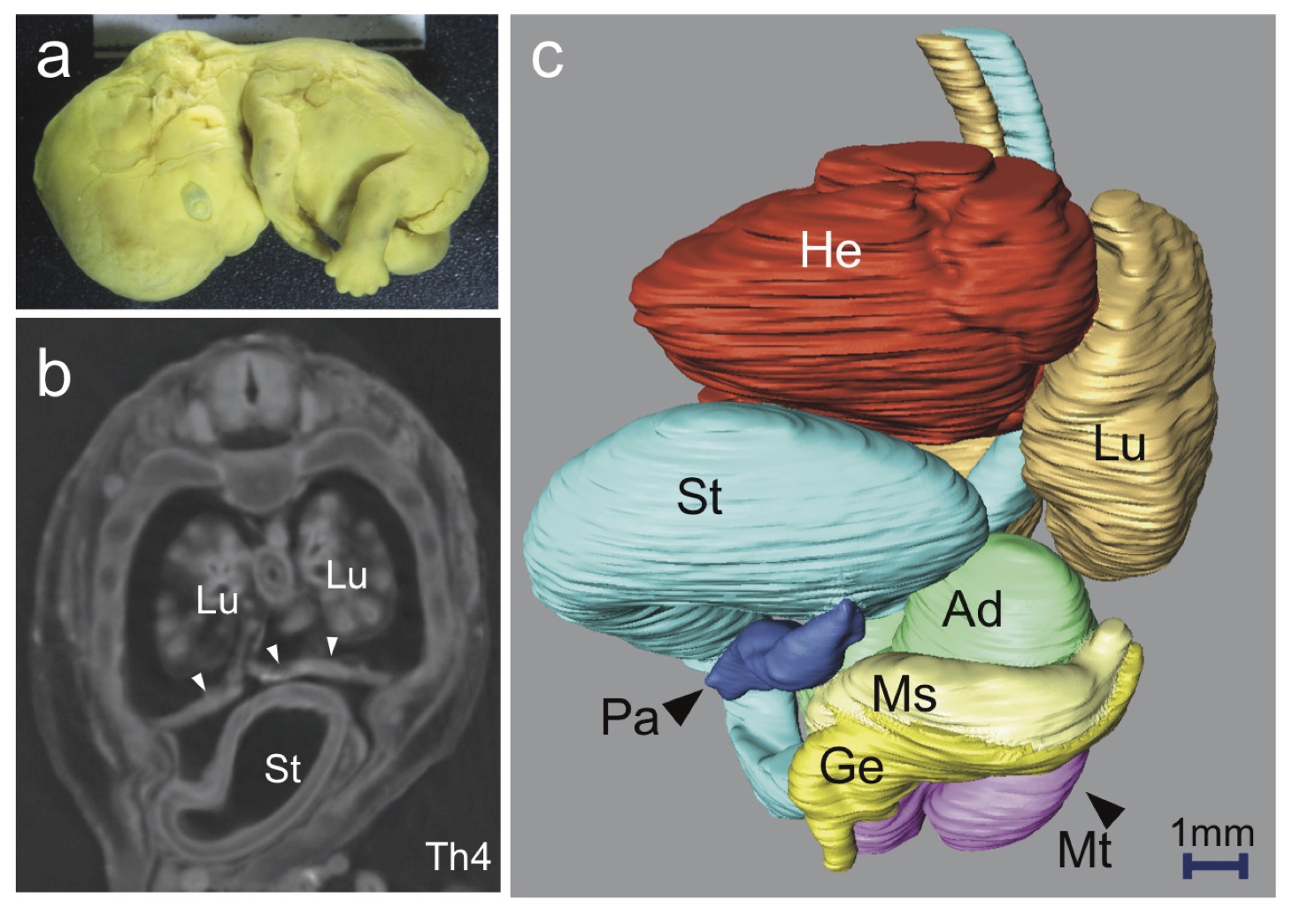
Figure 2: Representative embryos with liver abnormality (liver agenesis). a External view of the embryo at CS21, which shows no obvious external abnormality. b Phase-contrast X-ray computed tomography (PXCT) transverse sections at the level of Th4. No liver (Li) was detected in the plane sections, while the stomach (St) was observed in the midsagittal transverse sections at Th4. The diaphragm is indicated by arrow heads. Lung (Lu). c Left anterior oblique view of the three-dimensional (3-D) PXCT reconstruction of the embryo using Amira software (Visage Imaging, Berlin, Germany), demonstrating the locations of all intrathoracic, retroperitoneal, and intra-abdominal organs. The findings of note were as follows: agenesis of the liver; the stomach was deviated ventrally and cranially; the pancreas (Pa) was deviated ventrally; and the right mesonephros (Ms) and genital ridge (Ge) were absent. Adrenal gland (Ad), metanephros (Mt), and heart (He).
A representative embryo with liver agenesis is shown in Fig. 2. The size and gestational age were within the normal range for the embryo at CS 21. Obvious damage to, or anomalies of, the external forms were not present (Fig. 2a). The liver at CS21 usually occupies a large space in the abdominal cavity, which has a smooth surface due to the contact between the cranial surface and the diaphragm, and between the ventral surface and the abdominal wall [7]. In the present embryos, the liver was not detected in any of the serial plane sections (Fig. 2b). The locations of all intrathoracic, retroperitoneal, and intraabdominal organs were reconstructed in three dimensions (Fig. 2c). The absence of the liver had affected the locations of the other internal organs, especially the stomach, duodenum, and pancreas. The stomach was observed on the midsagittal line in the Th4 transverse sections, indicating that the stomach had deviated cranially and ventrally. The diaphragm was apparent in these sections.
The present study demonstrates that PXCT may be considered a powerful tool for visualization of internal structures of embryos, and for the detection of novel abnormalities during the embryonic period, without the need for histological analysis. The noninvasive and nondestructive properties of the technique are important for analysis of scarce specimens, such as human
embryos. The present study is the first step toward elucidating the latent abnormalities that result in spontaneous abortion in externally normal embryos [8].
REFERENCES
[1] K. Shiota, Congenital Anomalies 31, 67 (1991). [2] R. O’Rahilly and F. Müller, Developmental stages in human embryos: including a revision of Streeter’s” horizons” and a survey of the Carnegie Collection, (Carnegie Institution of Washington Publishing. 1987). [3] H. Nishimura, K. Takano, T. Tanimura and M. Yasuda, Teratology 1, 281 (1968). [4] K. Shiota, S. Yamada, T. Nakatsu-Komatsu, C. Uwabe, K. Kose, Y . Matsuda, T . Haishi, S. Mizuta and T . Matsuda, Am J Med Genet A 143A, 3121 (2007). [5] T. Takakuwa, Antat Rec (2017), in press. [6] A. Yoneyama, S. Yamada and T. Takeda, Fine Biomedical Imaging Using X-Ray Phase-Sensitive Technique, eds. G. D. Gargiulo and A. McEwan, Advanced Biomedical Engineering 107 (2011).
[7] A. Hirose, T. Nakashima, S. Yamada, C. Uwabe, K. Kose and T. Takakuwa, Anat Rec 295, 51 (2012).
[8] T. Kanahashi, S. Yamada, M. Tanaka, A. Hirose, C. Uwabe, K. Kose, A. Yoneyama, T. Takeda and T. Takakuwa, Anat Rec 299, 8 (2016).
Herniation into the extraembryonic coelom and return to the abdominal coelom
Background
PUH occurred independent of the liver.
Drastic changes occur during the development of the intestinal loop (IL), including physiological umbilical herniation (PUH) and its return. The present study was designed to analyze such developments three-dimensionally during human embryonic and early fetal period.
Materials and Methods
The software AMIRA was used to analyze the 3D digitalized data (high-resolution MRI, phase-contrast X-ray CT) obtained from the Kyoto Collection.
Results and Discussion
Based on the results of our analysis, the following time line and main features of IL formation were revealed:
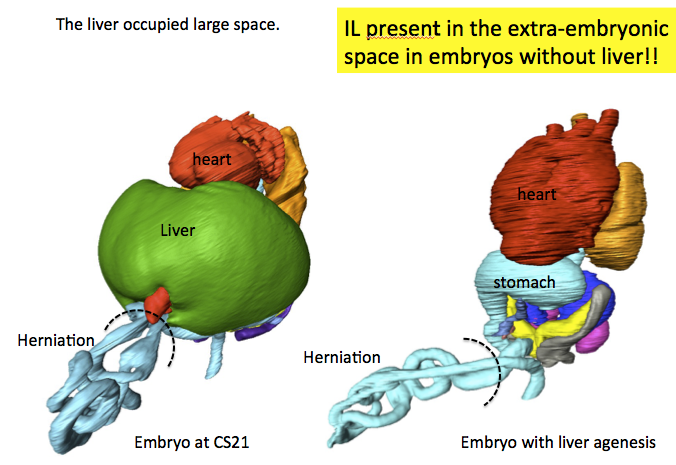
Herniate phase (Carnegie stage (CS)14-CS23, Crown-rump length (CRL) < 35 mm): IL rotation was initially observed as a slight deviation of the duodenum and colorectum from the median plane up to CS16. The PUH was noticeable after CS16. The IL displayed a hairpin-like structure, with the superior mesenteric artery (SMA) running parallel to the straight part and the cecum located to the left at CS18. The IL rotated around the SMA only during the early stages (until CS19). The IL gradually moved away, running transversely after CS19. Embryos with liver malformation showed PUH, which indicated that PUH occurred independent of liver volume.
Transition phase (CRL = 37, 41, and 43 mm): Intestinal return began from proximal to distal part in samples with CRL of 37 mm. The cecum returned before the distal end of the small intestine (ileum) in samples with CRLs of 41 and 43 mm.
Return phase: The cecum immediately reached its final position in the right lower quadrant of the abdomen (the adult position). The anti-clockwise “en-bloc rotation” described by descent and fixation of the cecum in the abdominal cavity may not exist. A rapid increase in the space available for the intestine in the abdominal coelom that exceeded the intestinal volume in the extraembryonic coelom was observed. The height of the umbilical ring increased in a stepwise manner between the transition and return phases and its height in the return phase was comparable to or higher than that of the hernia tip during the herniation phase. We speculated that the space is generated to accommodate the herniated portion of the intestine, similar to the intestine wrapping into the abdominal coelom as the height of the umbilical ring increases.
Conclusion
The data obtained in the present study demonstrate the precise timeline of IL formations, which indicate several points of discrepancy in the results of previous studies.
References
Nagata A, Hatta S, Imai H, Yamada S, Takakuwa T. Position of the cecum in the extraembryonic and abdominal coelom in the early fetal period. Congenit Anom 2019, in press.
Nagata A, Hatta S, Ji X, Ishikawa A, Sakamoto R, Yamada S, Imai H, Matsuda T, Takakuwa T. Return of the intestinal loop to the abdominal coelom after physiological umbilical herniation in the early fetal period. J Anat, 2019, 234, 456-464.doi: 10.1111/joa.12940.
Kanahashi T, Yamada S, Yoneyama A, Takakuwa T. Relationship Between Physiological Umbilical Herniation and Liver Morphogenesis During the Human Embryonic Period: A Morphological and Morphometric Study. Anat Rec 2019 in press.
Ueda Y, Yamada S, Uwabe C, Kose K, Takakuwa T, Intestinal rotation and physiological umbilical herniation during the embryonic period, Anatomical Record 299, 197-206, 2016, DOI: 10.1002/ar.23296
To obtain 3D digital data on early human development, we used some micro-imaging modalities such as magnetic resonance microscopy (MRM), episcopic fluorescence image capture (EFIC), and phase-contrast X-ray computed tomography (PXCT).
2.1 Magnetic resonance microscopy (MRM)
MR microscopy is a very powerful tool for 3D measurements of human embryos, because chemically fixed human embryos contain large quantities of mobile or NMR visible protons, which are major components of the formalin preservation fluid. MR imaging is nondestructive and does not need sectioning of embryonic tissues. Using MRM equipped with superconducting magnets ranging from 1.0T to 7.0T, embryos from the Kyoto Collections were imaged (Haishi et al., 2001, Matsuda et al., 2007, Matsuda et al., 2003, Yamada et al., 2010). The first super-parallel MR microscope was implemented on a 1.5 T clinical MRI scanner operated at University Hospital of Tsukuba University.
Kyoto Human Embryo Visualization Project (BIRD project); this is a collaborative research with Prof. Katsumi Kose of Tsukuba University and has been funded by the “Bioinformatics R & D (BIRD)” Project of the Japan Science and Technology Agency (2005-2010). Kyoto and Tsukuba Universities began a project in 1999 to acquire 3D MR microscopic images of thousands of human embryos using a super-parallel MR microscope operated at 2.35T (Shiota et al., 1991; Matsuda et al., 2003, 2007; Yamada et al., 2006). We were successful in acquiring high-resolution sectional images and in identifying the detailed structures of major organs. A database of developing human embryo images was established for future biomedical research (http://bird.cac.med.kyoto-u.ac.jp). This database will be useful not only in the study of human embryology but also for future gene mapping studies in human development.
Kose and his coworkers (Matsuda et al., 2003) developed a four-channel MR microscope with four unshielded gradient coil probes. The four-channel array probe was developed for a 2.35 T superconducting magnet. Each gradient coil probe consists of a rigid aluminum square frame [18 cm (W) × 20 cm (H) × 28 cm (D)] and slide planes made of thin brass plates (0.3 mm thick) acting as an RF shield. The RF coil units are exchangeable, and the diameter can be optimized for a given sample size. In the project, 18 mm diameter four-turn solenoid coils were used for the 100 MHz signal excitation and detection frequency. The pulse sequence was a T1-weighted 3D gradient echo sequence (TR = 100 ms, TE = 8 ms). Embryo specimens were imaged in test tubes (ID = 13.5 mm) filled with 4% formaldehyde solution. Introduction of a superconducting magnet (2.35 T) to MR microscopy significantly improved the quality of the MR images. The resolution was equivalent to that of low-magnification histological sections. The resolution now approaches 80 µm, and it is possible to identify various embryonic structures, such as the brain (and cerebral cortex), eyes, inner ears, pituitary gland, bronchi, lungs, stomach and intestines, kidneys, gonads, liver and spleen in embryos that are less than 30 mm in length. While introduction of a super-parallel MR microscope enabled imaging of 4-8 specimens simultaneously and significantly reduced the time required (Matsuda et al., 2003).
MRI (7T); MR images were acquired using a 7T MR system (BioSpec 70/20 USR; Bruker Biospin MRI GmbH; Ettlingen, Germany) with a 35-mm-diameter 1H quadrature transmit-receive volume coil (T9988; Bruker Biospin MRI GmbH). The 3D T1-weighted images were acquired using a fast, low-angle shot pulse sequence with the following parameters: repetition time, 30 ms; echo time, 4.037–6.177 ms; flip angle, 40°; field of view, 22.5 × 15.0 × 15.0–42.0 × 28.0 × 28.0 μm3; matrix size, 636 × 424 × 424–768 × 512 × 512; spatial resolution, 35.4–54.7 μm3.
It is feasible to apply MR microscopic imaging to fast and efficient screening of embryos in genetic and teratological studies by identification of internal visceral anomalies quickly, efficiently. MRI is nondestructive and does not need sectioning of specimens, which not only saves time and labor, but also allows precious specimens to remain intact.
Phase-contrast X-ray computed tomography (PXCT) is a relatively newer technique of imaging. In this imaging, the X-rays are used as electric waves which has the information of amplitude and phase. When an X-ray passes through a sample, their amplitude is decreased and phase is shifted. Conventional X-ray imaging (radiography) is based on absorption-contrast (i.e. amplitude imaging) and represents the mass-density distribution of X-ray inside the sample. The sensitivity is not sufficient to perform detailed observations of samples consisting of light elements such as biological soft tissues such as embryos without contrast agent or high X-ray dosages. In contrast, PXCT uses the phase-shift, occurring when X-rays pass through samples (Momose and Fukuda 1995). The sensitivity of the phase shift for light elements such as hydrogen, carbon, nitrogen, and oxygen is about 1000 times larger than that of absorption (Momose and Fukuda, 1995). For phase-shift detection, it is essential to convert the phase shift into the change in X-ray intensity. 2D and 3D observations of various biomedical samples have been performed using synchrotron radiation. The devices using this principle have been developed (Becker and Bonse, 1974, Yoneyama et al., 2004). The 3-D PXCT images of the human embryos were acquired using a radiographic imaging system (BL14-C, 17.8 keV) from Photon Factory, Institute of Materials Structure Science, High Energy Accelerator Research Organization (KEK, Tsukuba, Japan). The data provide a resolution of 18 μm/pixel or better by imaging systems with a two-crystal X-ray interferometer
Hideo Nishimura, Prof. in the Department of Anatomy at Kyoto University School of Medicine, instigated a collection of human conceptuses in 1961. Induced abortions were then legal in Japan under the Maternity Protection Law of Japan. Therefore, pregnancies were terminated for social reasons during the first trimester in a great majority of cases. The Congenital Anomaly Research Center was founded at Kyoto University, School of medicine in 1975, when the number of specimens reached over 36,000. The embryo collection comprises over 45,000 specimens nowadays, which represents the largest human embryo collection in the world.
Over 70% of the embryos were collected in the 1960s and 25.5% in the 1970s. The less than 5% of the specimens joined KC between 1980 and 1999 (Kameda et al, 2011). The specimens were collected from a total of 22 prefectures in six different districts; Kansai, Tokai, Hokuriku, Kanto, Chugoku/Shikoku with aid of approximately 1400 obstetrician.
1.2. How were so many samples collected?
The majority of the specimens were obtained after termination of pregnancy by dilatation or curettage during the first trimester for socioeconomic reasons. Other specimens resulted from spontaneous or threatened abortions. Dilatation and curettage (therapeutic abortions) given to healthy women enabled acquisition of undamaged, intact embryos. Approximately 20% of the specimens are undamaged, well-preserved embryos.
When the aborted materials were brought to our laboratory, the embryos were measured, staged, and examined for gross external abnormalities and presence of intrauterine death under a dissecting microscope. The developmental stage of the embryos (Carnegie stage: CS) was determined according to the criteria proposed by O’Rahilly and Müller (1987). Most of the specimens are between the CS13 and CS23, which is the critical period of teratogenesis. The specimens were fixed in 4% formaldehyde or Bouin solution and stored in 4% formaldehyde.
1.3. Feature of Kyoto Collections
Since the attending obstetricians were not involved in examining the aborted materials, Embryos were collected in a random manner. The collection of embryos was not biased by their outcome (e.g., normal or abnormal, live or dead), thus, the embryo collection is considered representative of the unbiased total intrauterine population in Japan (Nishimura, 1974, 1975, Shiota 1991) Using this representative embryo population, it was reported that the incidence of malformations in embryos were more frequent than that in infants (Nishimura et al., 1968), and that embryos with severe malformations were prone to spontaneous abortion at high rates (Shiota, 1991).
2) KC comprises embryo specimens with a large variety of external malformations as reported by previously published studies (Nishimura et al. 1968; Matsunaga and Shiota 1977; Yamada et al. 2004). Approximately 7.8% of the embryos exhibit external anomalies and 92.2% are without anomalies, which provide a unique opportunity to study the early stages of abnormal morphogenesis. The three most common anomalies were nuchal bleb, holoprosencephaly and spina bifida. Holoprosencephaly is encountered much more frequently (1/250 or more) in the unselected early human embryonic population (Matsunaga and Shiota, 1977).
3) Well-preserved samples were stored and some of them were selected to be sectioned serially; a total of 500 normal embryos and 500 abnormal embryos were stored as complete serial sections, including HPE embryos. All histological sections comprised in the library is plan to be digitalized. The project is currently focusing on serial sections of normal embryos. Parts of the digitized serial sections are accessible from our website (http://atlas.cac.med. kyoto-u.ac.jp).
4) Most specimens were collected along with detailed clinical and epidemiological information on the associated pregnancies and the mothers. These data were accumulated in the formats of paper sheets and punch cards. All data gathered in KC were turn into dizitalized textual and imaging data recently (Kameda et al 2011).
1.4 Ethics and legal point of view
The embryo specimens of KC were collected and stored legally and ethically in Japan in the first place.
After World War II, a lot of laws were established in Japan to reconstruct the country. The Eugenic Protection Law was one of such laws, and established in 1948. Revision of the law in 1952 made artificial abortion in early periods of pregnancy legally available by the articles as same as present Maternal Protection Law. Prof. Nishimura explained in his book about the rationale of this human embryo collection by “Japanese Eugenic Protection Law in 1952 (Nishimura 1975). The legal basis for artificial abortion in found in the 1st item of article 14 in Chapter III (Protection of the mother’s life and health) of the law as cited as follows (Nishimura 1966); ‘The physician designated by the Medical Association, which is a corporate juridical body established in the prefectural district as a unit, may exercise artificial interruption of pregnancy, at his discretion, on the person, who falls under any of the following items with consent of the person in question and the spouse: First item: A mother, whose health may be affected seriously by continuation of pregnancy or by delivery from the physical view point or economically’ (Nishimura 1966). Thus, in Japan, a lot of operations of artificial abortion have been performed for the reasons of economical reason. After the operation, embryo and placenta (or decidua) were taken out from maternal body and small embryos before 12 weeks of gestation and placenta were usually disposed as hospital waste. Prof. Nishimura planned to use the human embryo and placenta disposed as hospital waste for the research to elucidate the nature of embryonic morphology. He and his colleagues solicited the cooperation of the obstetricians who explained to their clients the significance of medical research and the contributions the parents could make by leaving the embryos with them. In most cases the mothers acceded to the requests of the obstetricians in whom they had trust. In addition, we regarded ourselves as an extension of the obstetrician’s clinic and could accept the specimens in good faith. The embryos were transferred to our laboratory with their some information such as date of operation, gestational ages, etc., but had no identifying information and cannot be linked to the parents or any relatives. Thus, the operations of artificial abortion could only be performed under the reasons based on the law, with the consent of mother and/or the father. The scientist or obstetrician could force mothers neither to take operation and nor to give the embryo to the scientist or obstetrician.
Therefore, the embryos have been obtained ethically. It is not appropriate to treat the Kyoto Collection and victims of Holocaust. Based on these backgrounds, our research have been approved by IRB of Kyoto University (The Committee of Medical Ethics of Kyoto University Graduate School of Medicine, Kyoto: E986, G377).
Three-dimensional (3D) analysis of the human embryonic and early-fetal period has been performed using digitized datasets obtained from the Kyoto Collection, in which the digital datasets play a primary role in research. Datasets include magnetic resonance imaging (MRI) acquired with 1.5 T, 2.35 T, and 7 T magnet systems, phase-contrast X-ray computed tomography (CT), and digitized histological serial sections. Large, high-resolution datasets covering a broad range of developmental periods obtained with various methods of acquisition are key elements for the studies. The digital data have gross merits that enabled us to develop various analysis. Digital data analysis accelerated the speed of morphological observations using precise and improved methods by providing a suitable plane for a morphometric analysis from staged human embryos. Morphometric data are useful for quantitatively evaluating and demonstrating the features of development and for screening abnormal samples, which may be suggestive in the pathogenesis of congenital malformations. Morphometric data are also valuable for comparing sonographic data in a process known as “sonoembryology.” The 3D coordinates of anatomical landmarks may be useful tools for analyzing the positional change of interesting landmarks and their relationships during development. Several dynamic events could be explained by differential growth using 3D coordinates. Moreover, 3D coordinates can be utilized in mathematical analysis as well as statistical analysis. The 3D analysis in our study may serve to provide accurate morphologic data, including the dynamics of embryonic structures related to developmental stages, which is required for insights into the dynamic and complex processes occurring during organogenesis
Abstract-The three-dimensional (3D) observations are required for analyzing complex morphogenetic processes that occur during human embryonic development. Serial histological sections were utilized not only for histological two-dimensional observation, but also for designing three-dimensional (3D) plaster or wax models, which enable the 3D changes to be visible, since the late nineteenth century. Analysis using the histological sections is the main approach that is developed in the recent studies. Additionally, imaging modalities, such as magnetic resonance imaging and phase contrast X-ray computed tomography, have been applied to embryology. High-resolution 3D datasets with an adequately large number of samples, covering a broad range of developmental periods with various methods of acquisition, are key features for the research. These datasets have the advantage of morphology, morphometry, and quantitative analysis using 3D coordinates. In particular, an adequate sample size is required for quantitative analysis using statistical methods and multidisciplinary computational anatomy (MCA) based analysis, which are expected to be useful analyzing methods for many unresolved tasks, such as quantitative movement (differential growth), branching morphogenesis, and information concerning physical and structural property. As a future perspective, analysis targets using digital imaging data may shift from embryonic period to early-fetal period (9-12 weeks after fertilization), which can apply to prenatal diagnosis using ultrasound. This data will timely contribute to improvements in prenatal diagnostics by detailing and comparing suitable markers for estimating developmental growth.
Three-dimensional analysis of human development using histological sections
Research for human embryology has been initiated since the late nineteenth century [1,2]. The morphological observations of human embryonic samples were the main approaches, including observation of the gross view, dissection, and histological sectioning. Classical embryology using histological techniques previously revealed a large number of morphological features according to the developmental stages and significantly contributed to the understanding of human development. Complex morphogenetic processes occur during embryonic development, which demanded the three-dimensional (3D) observations expanding to large areas. The 3D analyses using histological sections become the main approaches, which enable the 3D changes to be visible. Serial histological sections were not only utilized for histological two-dimensional observation, but also applied to design 3D plaster or wax models. The work of a team of scientists and technical specialists, such as illustrators and modelers, was established for development of human embryology. The historical models of Ziegler, Blechshmidt, and Heard are famous worldwide and are indispensable in research and teaching [3].
The 3D analyses using histological sections advanced with the advent of new technology. These include acquisition systems for digitalization of the samples, higher specification computers, and higher volume of storage. The digitized materials are primarily used for education and assistance of research, as they are attractive materials for students and researchers who could be apprehensive. They are also useful for database and references for the researches [4,5]
Using nearly 15,000 digitalized histological sections of the renowned Carnegie Collection of human embryonic specimens, de Bakker et al (2016) [6] created a 3D digital atlas and database featuring the first 2 months of human development. They identified and labeled up to 150 organs and structures per specimen and made 3D models to quantify growth, establish changes in the position of organs, and clarify current ambiguities. The 3D portable document formats of the reconstructions, and original and labeled images, are freely available (http://3datlasofhumanembryology.com).
Using whole-mount immunostaining, 3D imaging of solvent-cleared organ clearing and light-sheet imaging, Belle et al (2017) [7] generated a precise cellular and molecular cartography, a 3D cellular map of the human embryonic development during the first trimester of gestation. They provided high-resolution 3D images of the developing peripheral nervous, muscular, vascular, cardiopulmonary, and urogenital systems. Their work paved the way for a cellular and molecular reference atlas of human cells. All their 3D datasets are made available on a dedicated website (https://transparent-human-embryo.com/).
For an administrator of human embryo collections, the digitization of the histological glass slides is one solution for preserving the collections and for decreasing the maintenance cost. The Digital Embryology Consortium, an international partnership, was established in 2014 to digitize, preserve, and disseminate the major embryology histological collections for researchers (https://embryology.med.unsw.edu.au/embryology/index.php/Digital_Embryology_Consortium_-_Information) [8].
3D analysis of human development using imaging modalities in high resolution
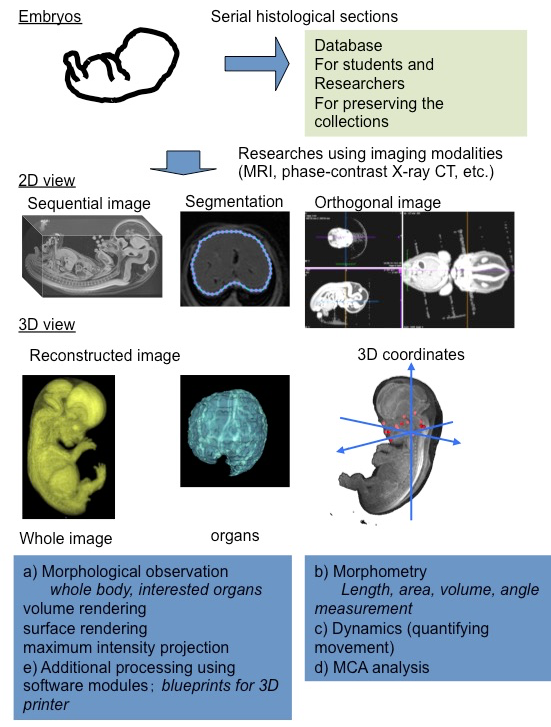
Figure 1. Three-dimensional analysis of human embryonic development, including organogenesis using digital datasets: outline.
Remarkable progress has been made in non-destructive imaging technologies, such as magnetic resonance imaging (MRI) and phase contrast X-ray computed tomography (CT), which have all been applied to embryology [9,10]. The imaging modalities are selected based on their destructive versus non-destructive features, the size of the samples, and the desired resolution.
Using MRI and ptychographic X-ray CT, our group proceeded the 3D analysis of human embryonic development, including organogenesis as research [11] (Figure 1). High-resolution 3D datasets with an adequately large number of samples, covering a broad range of developmental periods with various methods of acquisition, are key features for this research. These data sets have the advantage of morphology, morphometry, and quantitative analysis using 3D coordinates. In particular, an adequate sample size is required for quantitative analysis using statistical methods and PCA.
Morphological observations
The digital data had the following gross merits, which increased the efficiency of observations and accelerated the speed of morphological observations: 1) The data enabled us to analyze classical morphology and morphometry efficiently. 2) The complete 3D external and internal views and their reconstructions are easily obtained. 3) The obtained images can be resliced and rotated freely on the screen, by which the 3D shapes of the objects and their spatial relationships with the adjacent organs and tissues are easily recognizable. 4) The images from different embryos are simultaneously comparable on the screen. 5) Volume-rendering data can be utilized for advanced analysis.
Morphometry
Classical embryology using histological techniques provided little morphometric data [12,13]. For the measurement of spatial distances and angles between anatomical landmarks of interest, 3D reconstruction from serial histological sections was required. The procedure for such measurements was quite laborious with a number of possible issues that could arise, such as non-rigid deformation, tissue discontinuity, and accumulation of scale [A1] [14]. The digital data from MRI and CT have merit for morphometry. Precise morphometric data, length, angle, area, and volume of target regions and organs can be measured on the screen using digitalized data from MRI and CT images. Such morphometric data are useful for demonstrating the development features at each stage and for screening abnormally developed samples.
Quantitative analysis using 3D coordinates
A 3D coordinate can be given for each landmark by examining the position of the voxel on 3D digital data. Application of 3D coordinates of anatomical landmarks, especially MCA based analysis, are expected to be useful analyzing methods for many tasks, which remain to be dissolved as follows:
Quantitative movements (differential growth)
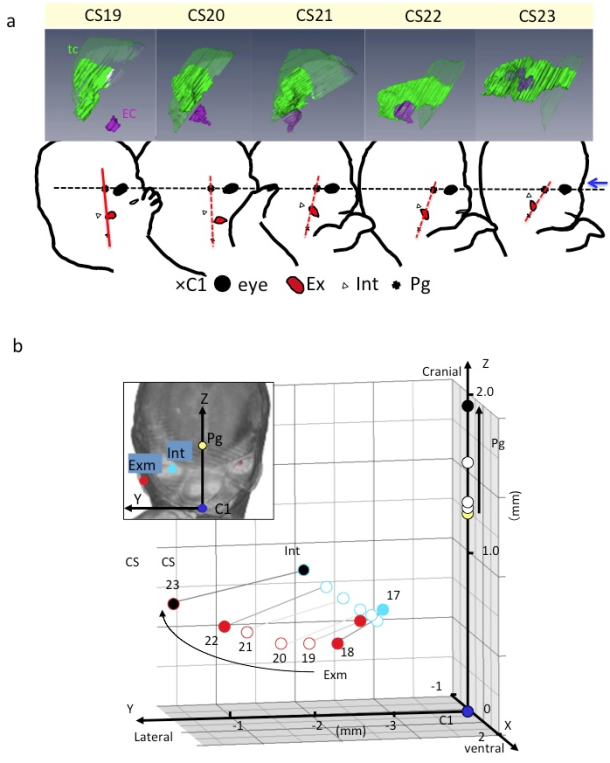
Figure 2. Three-dimensional analyses of quantitative movements (differential growth) A) Lateral view of embryos between Carnegie stage (CS) 19 and CS 23 showing the tympanic cavity and ear canal (upper) and craniofacial morphogenesis (lower). The ear canal (ec), external ear (Ex), eye (Ey), first cervical vertebra (C1), internal ear (int), pituitary gland (Pg), and tympanic cavity (tc). The dashed line indicates the reference axis connecting the middle point of the bilateral Ey and Pg (X-axis). The red line indicates the reference line connecting Pg and C1. Blue arrow indicates the frontal side of the face. Note that the Exm and Int are observed at similar position on the red segment. There is a gross change of angle between the black and red lines used. The change of angle may result from the formation of the mandibular apparatus and the structures at the base of the skull. B) Three-dimensional graph showing the relationship between the right external ear (Exm) and internal ear (Int) during development. Axes and anatomical landmarks are shown on frontal view of volume-rendering images. Abbreviations: Carnegie stage (CS), external ear (Exm), first cervical vertebra (C1). internal ear (int), pituitary gland (Pg)
Both the external and internal structures of embryos rapidly change in size and shape during the period of organogenesis. Many dynamic events are traditionally described as migration in which the position of structures changes from one region of the embryo to another. Gasser (2006) [15] recently demonstrated most of the positional changes of the developing structures, such as the sclerotome formation from the somite, the spinal ganglion formation from the neural crest, and the endocrine glands formation from the pharyngeal endoderm, which can be explained by differential growth.
For understanding the positional change of landmarks of interest and their relationships during development, the digitized data was advantageous for comparing structures of interest between different stages with identical magnification, superimposed on the same screen. The 3D positional change of interesting landmarks and their relationships during development were demonstrated [11,16-18], which indicated that many dynamic events can be explained by differential growth using 3D coordinates (Figure 2).
Shared mechanism for human organogenesis (Branching morphogenesis)
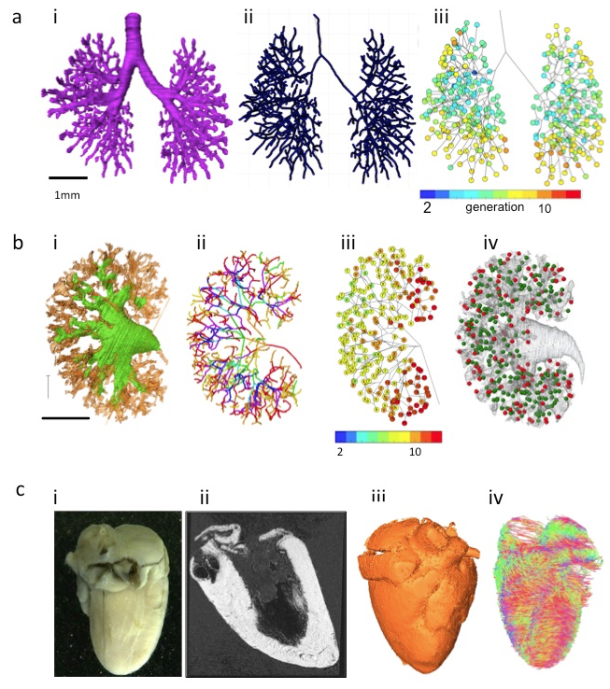
Organs, such as bronchi of the lungs, urinary collecting trees of the kidneys, the milk ducts of the mammary gland, develop from branched tubes during embryonic and fetal development. Because of many similarities between these branched tube structures, the shared mechanism was assumed. Recently, Hannezo et al (2017) [19] proposed a unifying theory to solve this issue. Namely, the certain tips stop growing in a random manner. For example, the branched mammary gland structures stop growing when the tips of the structure impinge on neighboring branches. In the kidney, this cessation has been proposed to occur when nephrons form near the end of the collecting ducts. The unifying theory mainly comes from experimental in vitro model or in vivo animal models. Analysis using human samples with 3D coordinates is awaited [20] (Figure 3AB).
Information concerning physical and structural property
Figure 3. Three-dimensional analysis using digitalized data acquired with imaging modalities A) Branching morphogenesis of the human bronchi during embryonic period (a) The bronchial tree was extracted from ptychographic X-ray computed tomography image. (b) Centerline of the bronchial tree was processed. (c) Generation number of each branch segments was indicated by colors. B) Branching morphogenesis of the human urinary collecting system (UCS) at Carnegie stage 23 (a) The UCS was extracted. (b) Centerline of the bronchial tree was processed. The tree was illustrated by rainbow colors from the proximal to peripheral branches. (c) Generation number of each branch segments was indicated by number and colors. (d) Position of nascent nephrons connected (green) and not connected (red) to UCS are shown. C) The fetal heart ex vivo (crown-rump length=94 mm) (a) The frontal gross view. (b) Magnetic resonance imaging (MRI)-T1 image. (c) The 3D volume-rendering image. (d) Diffusion tensor images MRI (DTI-MRI).
Imaging modalities data contain information not only regarding 3D morphology, but also regarding physical property. Diffusion tensor images MRI has also been applied to fetal brain [21] and cardiac muscles in mice [22,23]. The method is applicable to various organs and tissues that are anisotropic in nature (Figure 3C). Mesenchymal tissues consisting of fibers and membranous structures, such as the muscles, tendons, arteries, and bones, may be candidates for application of this method. These tissues have not been analyzed vigorously because of technical reason and their large target size.
Phase-contrast X-ray computed tomography with Zeff imaging methods can be used to recognize and differentiate heavy metals, such as iron, aluminum, nickel, and copper [24]. The 3D dynamics of such elements during human embryonic development are not currently known. Hematogenesis of the embryos may be also detectable using iron as a trace marker. This information with 3D distribution may provide new insight of human development.
Perspective
Shift from embryonic period to early-fetal period (9-12 weeks after fertilization)
The number of morphological studies on the early-fetal period (9-12 weeks after fertilization) is less as compared to that on the first 8 weeks after fertilization (at the end of Carnegie stage [CS] 23) [2] due to the several reasons. First, many researchers have been attracted to the dynamic morphogenesis in rather earlier developmental stages. Establishment of CS may contribute in encouraging studies for the early-fetal period. Second, it is difficult to apply histological analysis for the entire body of the fetus with a size larger than that at CS 23. Therefore, studies conducted on fetal period are mainly confined to localized histological analysis. The 3D datasets of larger samples corresponding to early-fetal period can be acquired with MRI in high resolution, which are worth analyzing as they can reveal the 3D development of the entire body and organs. Such morphometric data are also valuable for connecting and comparing the sonography data.
Application to prenatal diagnosis
The 3D information obtained in classical embryology since the late nineteenth century has been used as the basis of prenatal diagnosis using ultrasound (US). The use of US for prenatal diagnostics has rapidly increased in the past 30 years [25]. Moreover, 3D sonography performed with high-frequency transvaginal transducers has expanded as 3D sonoembryology, which provides a basis for assessing normal human development and can also be useful in detecting developmental anomalies [25,26].
Prenatal diagnosis using US enables a shift in diagnostics from the second trimester to the first trimester of gestation. At present, an embryo at 9 weeks after fertilization or younger can be assessed via morphological and morphometrical analyses, which corresponds to a CS of 15-16. While abnormal embryos younger than 12 weeks after fertilization are observed by chance for clinical indications, systematic screening using sonographic parameters results in the detection of abnormalities during the late first trimester (12-13 weeks after fertilization). Analysis using the digital data with MCA based method, during early-fetal period could timely contribute to improvements in prenatal diagnostics by detailing and comparing suitable markers for estimating growth and development [27].
References
Morgan LM. A social biography of Carnegie embryo no. 836. Anat Rec B New Anat. 2004; 276:3-7. doi: 10.1002/ar.b.20002.
O’Rahilly R, Muller F. Developmental stages in human embryos: including a revision of streeter’s horizons and a survey of the Carnegie collection. Washington: Carnegie Institution of Washington; 1987.
Smith BR. Visualizing human embryos. Sci Am. 1999; 280: 76-81. doi: 10.1038/scientificamerican0399-76.
Momose A, Takeda T, Itai Y, Hirano K. Phase-contrast X-ray computed tomography for observing biological soft tissues. Nat med. 1996; 2: 473-5. doi: 10.1038/nm0496-473.
Takakuwa T. 3D analysis of human embryos and fetuses using digitized datasets from the Kyoto Collection, Anat Rec. 2018; 301:960-9. doi: 10.1002/ar.23784
O’Rahilly R, Müller F. Developmental stages in human embryos: revised and new measurements. Cells Tissues Organs. 2010; 292:73-84. doi: 10.1159/000289817.
Levitan ML, Desmond ME. Expansion of the human embryonic brain during rapid growth: area analysis. Anat Rec. 2009; 292:472-80. doi: 10.1002/ar.20882.
Kajihara T, Funatomi T, Makishima H, Aoto T, Kubo H, Yamada S, et al. Non-rigid registration of serial section images by blending transforms for 3D reconstruction. Pattern Recognition. 2019; 96: 106956. doi.org/10.1016/j.patcog.2019.07.001
Gasser RT. Evidence that some events of mammalian embryogenesis can result from differential growth, making migration unnecessary. Anat Rec B New Anat. 2006; 289:53-63. doi: 10.1002/ar.b.20092.
Kagurasho M, Yamada S, Uwabe C, Kose K, Takakuwa T. Movement of the external ear in human embryo. Head Face Med. 2012; 8:2. doi: 10.1186/1746-160X-8-2.
Katsube, M, Yamada, S, Yamaguchi Y, Takakuwa T, Yamamoto A, Imai H, et al. Critical growth processes for the midfacial morphogenesis in the early prenatal period. Cleft Palate-Craniofacial J. 2019; 56: 1026–37. https://doi.org/10.1177/1055665619827189
Ozeki-Satoh M, Ishikawa A, Yamada S, Uwabe C, Takakuwa T. Morphogenesis of the middle ear ossicles and spatial relationships with the external and inner ears during the embryonic period. Anat Rec. 2016; 299: 1325-37. doi: 10.1002/ar.23457.
Hannezo E, Scheele CLGJ, Moad M, Drogo N, Heer R, Sampogna RV, et al. A unifying theory of branching morphogenesis. Cell. 2017;171: 242–55. doi: 10.1016/j.cell.2017.08.026.
Ishiyama H, Ishikawa A, Kitazawa H, Fujii S, Matsubayashi J, Yamada S, et al. Branching morphogenesis of the urinary collecting system in the human embryonic metanephros, PLoS ONE 2018; 13: e0203623. doi: 10.1371/journal.pone.0203623
Huang H, Xue R, Zhang J, Ren T, Richards LJ, Yarowsky P, et al. Anatomical characterization of human fetal brain development with diffusion tensor magnetic resonance imaging. J Neurosci 2009; 29:4263-73. doi: 10.1523/JNEUROSCI.2769-08.2009.
Mekkaoui C, Porayette P, Jackowski MP, Kostis WJ, Dai G, Sanders S, et al. Diffusion MRI tractography of the developing human fetal heart. PLoS One. 2013 ;8:e72795. doi: 10.1371/journal.pone.0072795.
Angeli S, Befera N, Peyrat JM, Calabrese E, Johnson GA, Constantinides CA. High-resolution cardiovascular magnetic resonance diffusion tensor map from ex-vivo C57BL/6 murine hearts. J Cardiovasc Magn Reson. 2014; 16:77. DOI: 10.1186/s12968-014-0077-x
Yoneyama A, Hyodo K, Takeda T. Feasibility test of Zeff imaging using x-ray interferometry. Appl Phys Lett. 2013; 103:204108. https://doi.org/10.1063/1.4831773.
Blaas HG. Detection of structural abnormalities in the first trimester using ultrasound. Best Pract Res Clin Obstet Gynaecol. 2014; 28:341–53. doi: 10.1016/j.bpobgyn.2013.11.004.
Pooh RK, Shiota K, Kurjak A. Imaging of the human embryo with magnetic resonance imaging microscopy and high-resolution transvaginal 3-dimensional sonography: human embryology in the 21st century. Am J Obste Gynecol. 2011; 204: 77:e1–e16. doi: 10.1016/j.ajog.2010.07.028.
Kobayashi A, Ishizu K, Yamada S, Uwabe C, Kose K, Takakuwa T. Morphometric human embryonic brain features according to developmental stage. Prenat Diagn. 2016; 36:338-45. doi: 10.1002/pd.4786.
Abstract. During human development, both external and internal morphological features change dramatically. External features, including those on the body and limbs, provide a good basis for determining the staging of each developing embryo. The application of three-dimensional (3-D) sonography with high-frequency transvaginal transducers has expanded and now fosters 3-D sonoembryology, which provides a basis for assessing normal human development and can also be useful in detecting developmental anomalies. The quantitative data of standard morphology for each Carnegie stage (CS) and early fetal period is required for the evaluation of the body and limbs in clinically obtained data, to allow for better prenatal morphological diagnosis. Analysis of the skeletal system during the human embryonic and early fetal period based will be described, including the rib cage, shoulder girdle, pelvis, and femur. The data obtained may contribute to such evaluations.
Introduction
During human development, both external and internal morphological features change dramatically. External features, including those on the body and limbs, provide a good basis for determining the staging of each developing embryo. For example, flexion and extension of the body combined with the posture of the upper and lower limbs have been integrated into the Carnegie stage (CS), which is universally accepted for determining the staging of human embryos [1]. Although such qualitative external changes are well described in the literature, 3-D quantitative changes in the body and limbs have not been well analyzed. The application of 3-D sonography with high-frequency transvaginal transducers has expanded and now fosters 3-D sonoembryology, which provides a basis for assessing normal human development and can also be useful in detecting developmental anomalies [2,3]. Such technology could contribute to more accurate prenatal diagnoses as well as enable a shift in the diagnostic time window (from the second to first trimester). Under these circumstances, the quantitative data of standard morphology for each CS and early fetal period are required for evaluation of the body and limbs in clinically obtained data, to allow for better prenatal morphological diagnoses. In the present chapter, analysis of the skeletal system during the human embryonic and early fetal period will be described, including the rib cage, shoulder girdle, pelvis, and femur.
Methods
All human embryo and early fetal specimens used are stored at the Congenital Anomaly Research Center of Kyoto University [4,5]. The phase contrast X-ray computed tomography (PXCT) and magnetic resonance imaging (MRI) were used for 3-D data acquisition [6,7]. PXCT and MRI data from selected embryos were analyzed precisely as serial 2-D and reconstructed 3-D images using Amira software (version 5.5; Visage Imaging, Berlin, Germany). The 3-D coordinates were initially assigned by examining the voxel position on 3-D images, which were subjected to principal component (PC) analysis and procrustes analysis.
Results
Rib cage
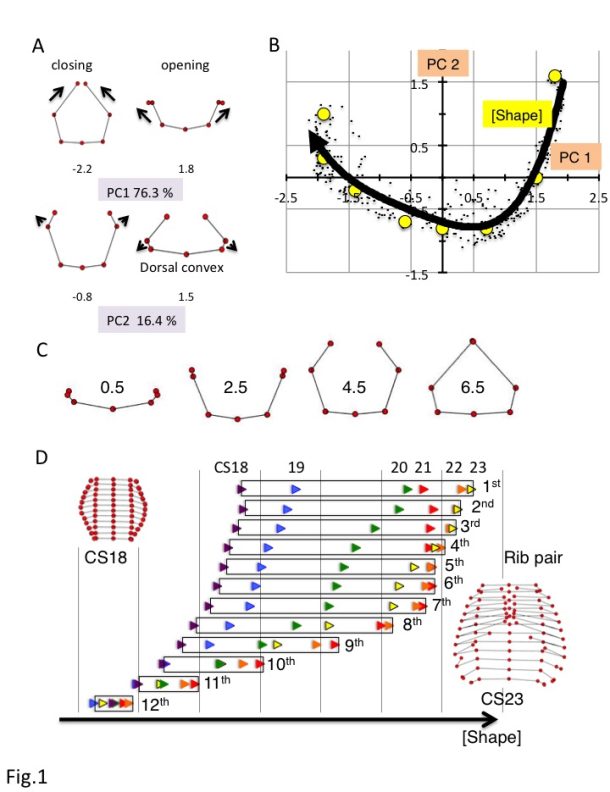
Fig. 14.1 Analysis of the rib cage based on MCA a) Changes in the ribs based on principal component analysis (PC) 1 and PC2. PC scores are indicated below each illustration. b) Scatter plot of PC1 and PC2 values for all rib pairs (n = 348). c) Rib morphologies for each F(Shape) value. d) Changes in F(Shape) according to rib number. CS18, purple; blue, CS19; green, CS20; red, CS21; orange, CS22; yellow, CS23.
The rib cage mainly consists of 12 pairs of ribs and vertebrae as well as the hypaxial muscles on the chest and upper abdominal parts of the body. In the early embryonic period until CS16, all visceral organs, such as the heart, lung, liver, and digestive tract, are covered with soft tissue. However, these organs are not protected by the rib cage because no cartilage or muscle formation is observed until CS16 [1,8]. Such organs are covered by the rib cage until the end of the embryonic period. The rib cage becomes detectable with cartilage formation at CS17, expanding outward from the dorsal side of the chest-abdominal region [9]. The ribs elongate progressively to surround the chest, differentiating into the upper and lower rib cage regions by CS20. The ends of the corresponding ribs in the upper region elongate towards each other, leading to their joining and sternum formation between CS21 and CS23, whereas the lower region of the rib cage remains widely open. The rib cage can be divided anatomically and functionally into the upper and lower thoracic regions. The upper region is related to the pulmonary part of the respiratory system and upper limbs, while the lower thorax is anatomically related to the diaphragmatic part of the respiratory system and also closer to the abdominal cavity and locomotor apparatus [10,11]. We aimed to analyze the morphogenesis of all ribs from the first to the twelfth rib pairs plus vertebrae to compare their differences and features according to the position along the cranial-caudal axis during the human embryonic period [12].
Seven rib cage landmarks, from the first to the twelfth vertebra, and the ribs (for a total of 84 landmarks) were located for each sample. A total of 384 sample data from 32 samples were subjected to process and principal component (PC) analyses, using MATLAB (R2017b, MathWorks, USA) software-assisted algorithms based on orthogonal coordinates of the voxels at each reference point. PC1 and PC2 accounted for 76.3% and 16.4% (sum, 92.7%) of the total variance, respectively, indicating that the change in shape was accounted for by two components (Fig.1A). Changes in PC1 resulted in a circular form surrounding the trunk. A decrease in PC1 showed closing of the rib tips, while an increase in PC1 showed opening of the rib tips. Changes in PC2 showed the movement of the lateral projection and dorsal convexity of the ribs. An increase in PC2 showed posterior movement of the lateral projection at the middle part of the rib, which is related to the dorsal convexity of the ribs, while a decrease in PC2 showed anterior movement of the lateral projection at the middle part of the ribs.
The distribution of scatter plots of the PC1 and PC2 values for each rib showed a fishhook-like shape (Fig.1B). The distribution was fitted to a quartic equation as follows: y = 0.072X4 + 0.1535X3 + 0.1785X2 – 0.2976X – 0.7001; R² = 0.82. PC1 and PC2 plots for each rib moved positions along the fitting curve according to the development of CS18 to CS23. The scatter plots moved in a wide range from the center right (quadrant IV) to the left, reached the left end (quadrant II) of the fitting curve, and moved slightly back in the upper ribs (1-7). However, the scatter plots moved in a narrower range from the center right to the center (quadrant IV) in the lower ribs. Movement was limited to the right (quadrant I) in the 11th and 12th ribs.
PC1 and PC2 values for each rib were plotted close to the fitting curve, for which the shape could be determined using a single parameter. We denote the fitting curve in the principal component subspace in Fig.1B by F(Shape), where Shape is the arc length parameter along the fitting curve and provides a linear scale for shape representation. Thus, the right end of the fitting curve (2.0,1.8) was designated as origin O of F(Shape), while the left end of the curve (-2.3, 1.0) was 6.6. PC1 and PC2 plots by rib x can determine the nearest point X on the fitting curve. The distance XO along the fitting curve was defined as the value of rib x for F(Shape).
F(Shape) = 0.5 showed that the paired ribs were on the dorsal side of the trunk with the opening of the rib tips (Figure 1C). F(Shape) = 2.5 showed that the paired ribs surrounded the dorsal side of the trunk with dorsal convexity of the ribs. The rib tips were separated. F(Shape) = 4.5 showed that the paired ribs had a circular form that surrounded more than half of the trunk, with the lateral projection at the middle part of the ribs. F(Shape) = 6.5 showed that the paired ribs had a circular form surrounding almost all of the trunk with the dorsal convexity of the ribs. The bilateral rib tips were almost closed. The change in F(Shape) at each rib pair is indicated. The development of each rib pair could be indicated as an increase in the F(Shape) scale in almost all conditions (Figure 1D). However, the development of a subset of rib pairs (1st-8th) resulted in a plateau or even decrease in the F(Shape) scale at the end of the embryonic period (between CS22 and CS23).
Our data clearly demonstrated that human embryonic ribs all progress through common morphological forms irrespective of their position on the axis. The data suggested that in a parsimonious model, the common series of rib pairs can be controlled by a small number of factors.
Femur
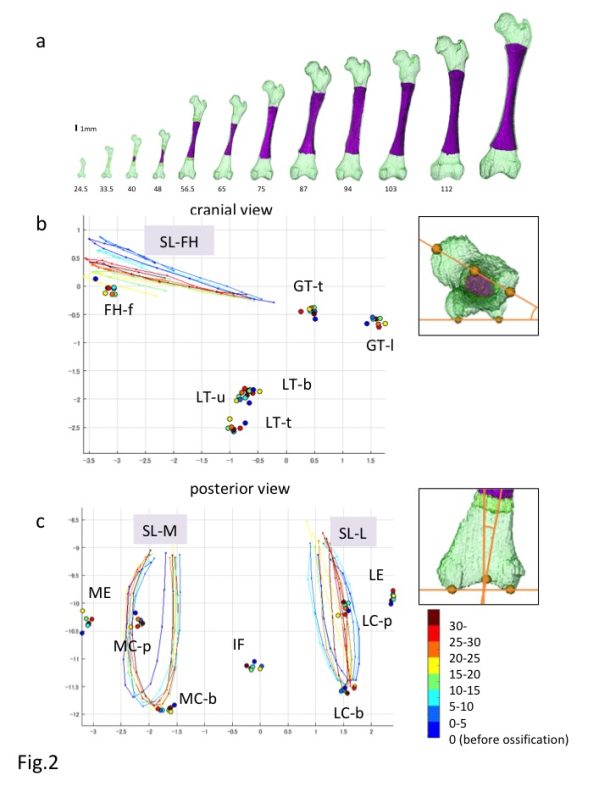
Fig. 14.2 Analysis of the femur based on MCA a) Reconstruction of the Femur during development b,c) Reconstructed Procrustes shape coordinates for the proximal (b) and distal (c) epiphysis of the fetal femur. FH-f: center of the femoral head fovea; GT-1: most lateral point of the greater trochanter; GT-t: top of the greater trochanter; IF: Intercondylar fossa; LC-b: lateral condyle (bottom); LC-p: lateral condyle (posterior); LE: lateral epicondyle; LT-b: bottom end of the lesser trochanter; LT-t: top of the lesser trochanter; LT-u: upper end of the lesser trochanter; MC-b: medial condyle (bottom); MC-p: medial condyle (posterior); ME: medial epicondyle; SL-FH: semi-landmarks from the upper end to the lower end of the femoral head along the plane passing through the midpoint of the femoral head, femoral neck, and greater trochanter; SL-L: semi-landmarks along the roundness of the lateral condyle from the upper end to the opposite side; SL-M; semi-landmarks along the roundness of the medial condyle from the upper end to the opposite side.
The femur is a long bone that develops via endochondral ossification. In particular, the human femur first appears as mesenchymal condensation between CS16 and CS17. Chondrification occurs between CS17 and CS18 and subsequently proceeds to endochondral ossification between CS22 and CS23 [1,8,13]. The cartilage structure influences bone structure formation, as the cartilage structure acts as the blueprint replaced by the bone structure. How the morphological features of the cartilage structure may be replaced by those of the bone structure has not been fully demonstrated, especially precise quantitative information regarding the 3-D formation of the femur.
The morphogenesis and internal differentiation process of the femur were analyzed in 3-D from the fetus (CRL11-185 mm, n = 62) [14]. Procrustes analysis was performed to distinguish the change in shape from the change in size according to growth using defined landmarks (n = 13) and semi-landmarks (n = 3). Centroid sizes at both the proximal and distal epiphyses showed a strong positive correlation with the ossified shaft length (OSL)(R2 = 0.99 and 0.99). The Procrustes shape coordinates for the proximal epiphysis indicated that each landmark on the greater and lesser trochanters and femoral head fovea was located in the same position irrespective of the OSL (Fig. 2A). In comparison, semi-landmarks at femoral head (SL-FH), which lined the femoral head, moved in accordance with the increase in OSL. Procrustes analysis indicated that changes in the femur shape after ossification were limited, and were mainly detected at the time of initial ossification and shortly thereafter. In contrast, femoral neck anteversion and torsion of the femoral head continuously changed during the fetal period. The Procrustes shape coordinates for the distal epiphysis indicated that each landmark was located in the same position irrespective of the OSL (Fig. 2B). semi-landmarks along the lateral and medial condyles (SL-L, SL-M) were located in different positions according to the OSL, although no obvious regularity was noted.
Torsion of the lower leg, including the femur (anteversion), was continuously observed during the fetal period and after birth [15-17]. Torsion of the femur may be affected by repetitive and persistent mechanical forces and the intrauterine position [3]. With respect to mechanical forces, muscle tension and local forces exert a rotary stress on the epiphysis. Remodeling at the metaphysis and epiphysis during the growth of a long bone such as the femur is well known as the mechanism that maintains the shape [8]. Anatomical landmarks remained in the same relative position during subsequent endochondral ossification in the present study, indicating that the remodeling system during femur shaft growth in the longitudinal direction is elaborate.
Shoulder girdle
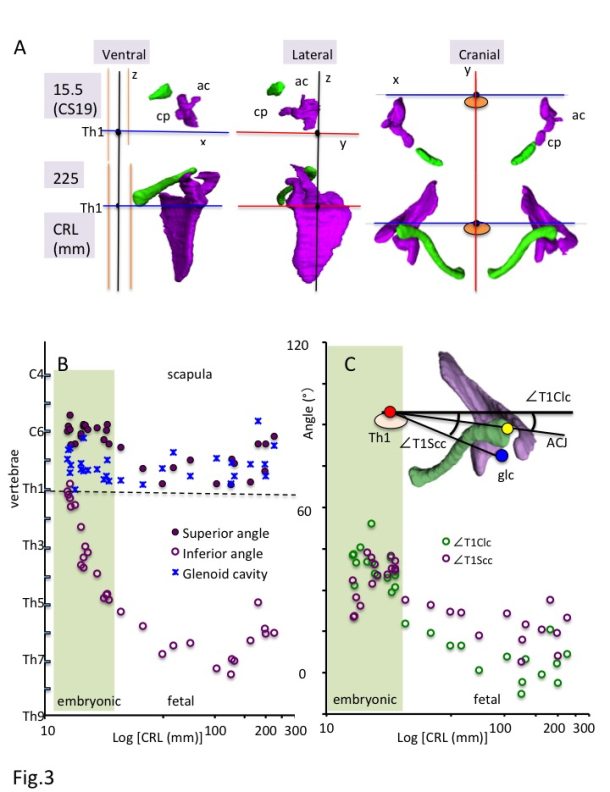
Fig. 14.3 Analysis of the shoulder girdle based on MCA a) Ventral, lateral, and cranial views of the 3-D reconstruction of the scapula (purple) and clavicle (green) in the embryonic (CS19) and fetal (CRL 225 mm) period. Th1: first thoracic vertebra; ac: acromion; cp: Coracoid process. b) Position of the scapula along z-axis. Solid purple circles indicate the superior angle of the scapula (spa), open purple circles indicate the inferior angle of the scapula (ifa), and blue stars indicate the center of the glenoid cavity (glc). c) Relationship between the scapula and clavicle from the cranial view. Solid yellow circles indicate the angles between the glc-Th1 and ACJ-Th1 segments from the cranial view (∠T1Scc-∠T1Clc).
The 3-D reconstruction and morphometry in our study revealed that all landmarks on the shoulder girdle remained at a similar height except the inferior angle, which means that the scapula enlarges in the caudal direction and reaches the adult position during the fetal period (Fig. 3A-B). The position of the shoulder girdle during the embryonic and fetal periods was unique (Fig. 3A and 3C). In contrast to the constant position of the clavicle, the scapula body was rotated internally and upward at the initiation of the morphogenesis. Thus, the scapula body of both seems almost parallel. The internal rotation of the scapula was changed externally, while the upward rotation remained unchanged. Compared with the adults, the scapula was still rotated internally and upward during the fetal period. The shoulder girdle is located in the ventral part of the body (vertebrae) during the initial morphogenesis, which changes the position to the lateral side of the vertebrae during the late embryonic period and fetal growth. The position during the fetal period may be consistent with that in adults. Such unique positioning of the shoulder girdle may contribute to the stage-specific posture of the upper limb, which is an important external feature for determining the staging, especially between CS18 and CS23 [1]. For example, the axial skeleton (vertebrae) becomes straight and the upper limb extends vertically to the axial skeleton at CS19. The shoulder (humerus head) becomes externally evident, and the joint flexed with the elbow is pronated at CS23. The posture may be explained, in part, by the unique positional change of the scapula during the embryonic period.
Conclusion
Skeletal system analysis may provide a useful standard for morphogenesis and morphometry of the skeletal system, which can serve as the basis to better understand embryonic and early fetal development and aid in differentiating normal and abnormal development.
References
O’Rahilly R, Muller F. Developmental stages in human embryos: including a revision of Streeter’s horizons and a survey of the Carnegie collection. Washington: Carnegie Institution of Washington; 1987.
Blaas HG. Detection of structural abnormalities in the first trimester using ultrasound. Best Pract Res Clin Obstet Gynaecol. 2014; 28:341–53. doi: 10.1016/j.bpobgyn.2013.11.004.
Pooh RK, Shiota K, Kurjak A. Imaging of the human embryo with magnetic resonance imaging microscopy and high-resolution transvaginal 3-dimensional sonography: human embryology in the 21st century. Am J Obste Gynecol. 2011; 204: 77:e1–e16. doi: 10.1016/j.ajog.2010.07.028.
Nishimura H, Takano K, Tanimura T, Yasuda M. Normal and abnormal development of human embryos: first report of the analysis of 1,213 intact embryos. Teratology. 1968; 1:281–90.
Yamaguchi Y, Yamada S. The Kyoto collection of human embryos and fetuses: history and recent advancements in modern methods. Cells Tissues Organs. 2018; 205:314–9. doi: 10.1159/000490672.
Yoneyama A, Yamada S, Takeda T. Fine biomedical imaging using X-ray phase-sensitive technique. In: Gargiulo G, editors. Advanced Biomedical Engineering. Rijeka: InTech; 2011. p 107–128.
Toyoda S, Shiraki N, Yamada S, Uwabe C, Imai H, Matsuda T, et al. Morphogenesis of the inner ear at different stages of normal human development. Anat Rec. 2015; 298:2081–90. doi: 10.1002/ar.23268.
O’Rahilly R, Müller F. The skeletal system and limbs. In: O’Rahilly R, Müller F, editors. Human Embryology & Teratology. 3rd ed. New York: Wiley-Liss; 2001. p 357–94.
Okuno K, Ishizu K, Matsubayashi J, Fujii S, Sakamoto R, Ishikawa A, et al. Rib cage morphogenesis in the human embryo: A detailed three-dimensional analysis. Anat Rec. 2019; 302: 2211-23, doi: 10.1002/ar.24226.
Bastir M, García-Martínez D, Recheis W, Barash A, Coquerelle M, Rios L, et al. Differential growth and development of the upper and lower human thorax. PLoS One. 2013; 8:e75128. doi: 10.1371/journal.pone.0075128.
García-Martínez D, Recheis W, Bastir M. Ontogeny of 3D rib curvature and its importance for the understanding of human thorax development. Am J Phys Anthropol. 2016; 159:423–31. doi: 10.1002/ajpa.22893.
Matsubayashi J, Okuno K, Fuji S, Ishizu K, Yamada S, Yoneyama A, et al. Human embryonic ribs all progress through common morphological forms irrespective of their position on the axis, Dev Dyn. 2019, 248, 1257-63, doi: 10.1002/dvdy.107.
O’Rahilly R, Gardner E. The timing and sequence of events in the development of the limbs in the human embryo. Anat Embryol. 1975;148: 1-23. doi: 10.1007/BF00315559.
Suzuki Y, Matsubayashi J, Ji X, Yamada S, Yoneyama A, Imai H, et al. Morphogenesis of the femur at different stages of normal human development, PLoS ONE. 2019;14: e0221569. doi: 10.1371/journal.pone.0221569.
Felts WJ. The prenatal development of the human femur. Am J Anat. 1954;94: 1-44. doi: 10.1002/aja.1000940102.
Guidera KJ, Ganey TM, Keneally CR, Ogden JA. The embryology of lower-extremity torsion. Clin Orthop Relat Res. 1994;302: 17-21.