






掛谷さんの修士論文がJ Anatomyに掲載されました。
発生途中、消化管は臍帯腔内に脱出し、CRL40mmころに短時間で還納されます。還納の仕方は、これまで消化管の動きを中心に研究されており、slide-stack model(消化管はループを形成したまま還納するというモデル)が優勢でした。本論文では、下記の2つの定説を覆す内容です。
- 消化管の臍帯内脱出の還納はCRL30mmころから時間をかけて行われること
- 消化管は臍帯輪通過時にはループが解除されていること
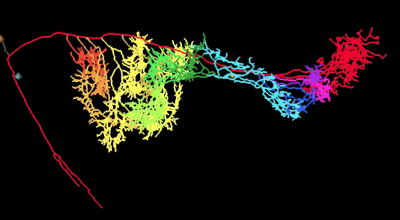
複雑な小腸の走行を追跡しても限界があることを認識し、この論文では消化管を栄養する上腸間膜動脈とその小腸枝の走行を正確に追うことで、還納経過中の小腸の位置や形状、走行をしめすとともに、血管系の分布、形状変化も示すことができました。還納は腸管の動きとして認識される時期に先行する血管系の位置の変化により開始され、これまでのコンセンサスよりも早く始まることを示しました。臍帯輪通過時には、消化管とそれを栄養する動脈の走行は形状を変えます。消化管はループがほどけ、臍帯輪を2本以上の消化管が通過することはありません。また、臍帯輪において消化管、腸間膜、動脈は整然とならび、どの個体でもほぼ一定です。
この組織だった配置は腸管への血行が安全に確保されるために必要とかんがえられます。
KakeyaM, Matsubayashi J, Kanahashi T, Männer J, Yamada S, Takakuwa T. The return process of physiological umbilical herniation in human fetuses: the possible role of the vascular tree and umbilical ring. J Anatomy 2022, 241(3), 846-859. https://doi.org/10.1111/joa.13720
Abstract
The human intestine elongates during the early fetal period, herniates into the extraembryonic coelom (EC), and subsequently returns to the abdominal cavity (AC). The process by which the intestinal loop returns to the abdomen remains unclear. This study aimed to document positional changes in the intestinal tract with the superior mesenteric artery (SMA) and branches in 3D to elucidate the intestinal loop return process (transition phase). Serial histological cross-sections from human fetuses (crown–rump length [CRL] range: 30–50 mm) in the herniation (n = 1), transition (n = 7), and return (n = 2) phases were selected from the Blechschmidt Collection. The distribution of the SMA trunk and all intestinal and sister branches entering the intestines was visualized so that positional changes in branches were continuous from the herniation to return phases. Positional changes in SMA branches proceeded in an orderly and structured manner; this is essential for continuous blood supply via the SMA to the intestine during transition and for safe intestinal return. Changes in the SMA distribution proceeded prior to the detection of initiation of intestinal tract return, which might start earlier and last much longer than our consensus (i.e., that the return of the herniated intestine begins when the CRL is approximately 40 mm and ends within a short time). In the cross-section of the umbilical ring in the herniation and transition phases, one proximal limb and one distal limb were observed with SMA intestinal branches, which were fully packed in the umbilical ring. The SMA branches were aligned from inferior to superior along the SMA main trunk. In the herniation phase, the distribution of 3rd–13th branches aligned from proximal inferior medial to distal superior left with a slight spiral in the EC, the tips of which suggested an orderly running course of the small intestine. In the transition phase, SMA branches running across the umbilical ring that fed the small intestine were observed, suggesting that the intestine was uncoiled and ran across the umbilical ring almost vertically. The estimated curvature value supported the phenomenon of uncoiling at the umbilical ring; the value at the umbilical ring was lesser than that in the AC and EC. During the transition phase, the proximal and distal limbs transversely ran side by side in the AC, umbilical ring, limbs on the cranial side, and mesentery on the caudal side. The SMA trunk and its branches ran in parallel, cranially to caudally aligned in the mesentery. This layout of the umbilical ring was maintained during the transition phase. In the return phase, the SMA trunk was gently curved from the upper left to the lower right of the AC; around 12 branches spread with a winding staircase appearance. The intestinal tract reached its definitive position immediately after all tissues crossed the umbilical ring and released any restriction. Each SMA branch and the corresponding region of the intestinal tract form a unit and change their position, though the conformation may change within each unit when running across the umbilical ring. We suggest that the slide–stack model requires revision.