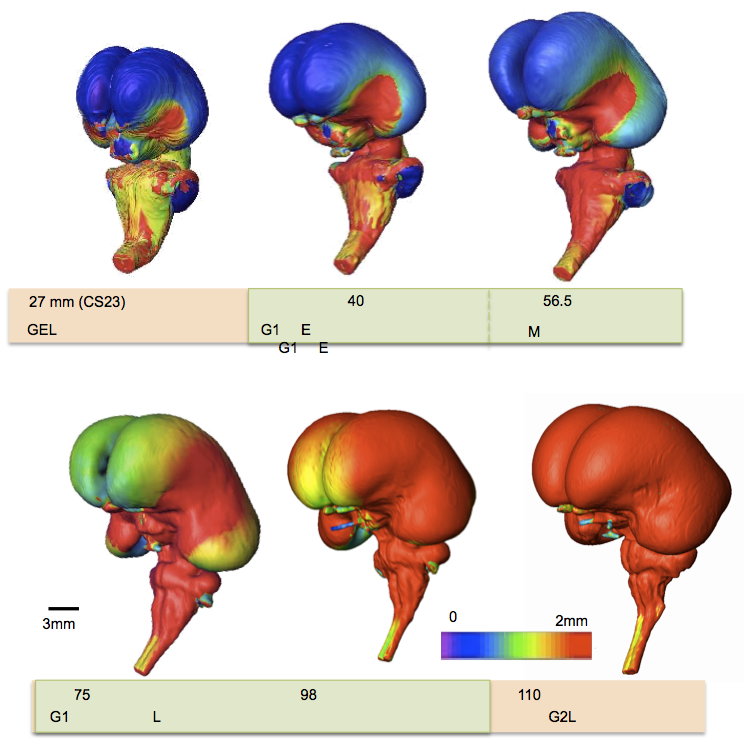
pSP-IZ の厚さは 3D で表示され、中外側領域で大きかった。CRL 64 mm)に、厚い領域は、島の原基の周りの外側、上部、および後部領域に拡大しました。
層構造は、発達初期に厚くなるのではなく、薄く成長して広がった。
Terashima, M., Ishikawa A., Männer J., Yamada S.&Takakuwa T. (2021) Early development of the cortical layers in the human brain. Journal of Anatomy, 239, 1039–1049. https://doi.org/10.1111/joa.13488
Abstract
The cortical plate (CP) first appears at seven postconceptional weeks (pcw), when it splits the preexisting preplate into two layers, the marginal zone and the presubplate (pSP). Although three-dimensional (3D) analysis using fetal magnetic resonance imaging and two-dimensional tissue observations have been reported, there have been no studies analyzing the early development of the layer structure corresponding to the pSP stage in 3D. Here, we reconstructed 3-D models of the brain with a focus on the cortical layers in pSP stage. To achieve this, we digitized serial tissue sections of embryos between CS20 and CS23 from the Kyoto Collection (n = 7, approximately 7–8.5 pcw), and specimens at early fetal phase from the Blechschmidt Collection (n = 2, approximately 9.5–12 pcw, crown rump length [CRL] 39 and 64 mm). We observed tissue sections and 3D images and performed quantitative analysis of the thickness, surface area, and volume. Because the boundary between pSP and the intermediate zone (IZ) could not be distinguished in hematoxylin and eosin-stained sections, the two layers were analyzed together as a single layer in this study. The histology of the layers was observed from CS21 and became distinct at CS22. Subsequently, we observed the 3-D models; pSP-IZ was present in a midlateral region of the cerebral wall at CS21, and an expansion centered around this region was observed after CS22. We observed it over the entire cerebral hemisphere at early fetal phase (CRL 39 mm). The thickness of pSP-IZ was visible in 3D and was greater in the midlateral region. At the end of the pSP stage (CRL 64 mm), the thick region expanded to lateral, superior, and posterior regions around the primordium of the insula. While, the region near the basal ganglia was not included in the thickest 10% of the pSP-IZ area. Middle cerebral artery was found in the midlateral region of the cerebral wall, near the area where pSP-IZ was observed. Feature of layer structure growth was revealed by quantitative assessment as thickness, surface area, and volume. The maximum thickness value of pSP-IZ and CP increased significantly according to CRL, whereas the median value increased slightly. The layer structure appeared to grow and spread thin, rather than thickening during early development, which is characteristic during pSP stages. The surface area of the cerebral total tissue, CP, and pSP-IZ increased in proportion to the square of CRL. The surface area of CP and pSP-IZ approached that of the total tissue at the end of the pSP stage. Volume of each layer increased in proportion to the cube of CRL. pSP-IZ and CP constituted over 50% of the total tissue in volume at the end of the pSP stages. We could visualize the growth of pSP-IZ in 3D and quantify it during pSP stage. Our approach allowed us to observe the process of rapid expansion of pSP-IZ from the midlateral regions of the cerebral wall, which subsequently becomes the insula.
大脳側面における大脳の比率 (長さ/高さ) と基準線に対する大脳の角度は、大脳の成長と C 字型の形成を反映している可能性がある。
これらの所見は、胎児期初期を細分化するための候補となる可能性がある。
52. Takakuwa T, Shiraishi N, Terashima M,Yamanaka M, Okamoto I, Imai H, Ishizu K, Yamada S, Ishikawa A, Kanahashi T. Morphology and morphometry of the human early fetal brain: A three-dimensional analysis. J Anatomy; 239 (2) 498-516, 2021, doi.org/10.1111/joa.13433
Abstract
Morphometric analyses in the early foetal phase (9-13 postconceptional week) are critical for evaluating normal brain growth. In this study, we assessed sequential morphological and morphometric changes in the foetal brain during this period using high-resolution T1-weighted magnetic resonance imaging (MRI) scans from 21 samples preserved at Kyoto University. MRI sectional views (coronal, mid-sagittal, and horizontal sections) and 3D reconstructions of the whole brain revealed sequential changes in its external morphology and internal structures. The cerebrum’s gross external view, lateral ventricle and choroid plexus, cerebral wall, basal ganglia and thalamus, and corpus callosum were assessed. The development of the cerebral cortex, white matter microstructure, and basal ganglia can be well-characterized using MRI scans. The insula became apparent and deeply impressed as brain growth progressed. A thick, densely packed cellular ventricular/subventricular zone and ganglionic eminence became apparent at high signal intensity. We detected the emergence of important landmarks which may be candidates in the subdivision processes during the early foetal period; the corpus callosum was first detected in the sample with crown-rump length (CRL) 62 mm. A primary sulcus on the medial part of the cortex (cingulate sulcus) was observed in the sample with CRL 114 mm. In the cerebellum, the hemispheres, posterolateral fissure, union of the cerebellar halves, and definition of the vermis were observed in the sample with CRL 43.5 mm, alongside the appearance of a primary fissure in the sample with CRL 56 mm and the prepyramidal fissure in the sample with CRL 75 mm. The volumetric, linear, and angle measurements revealed the comprehensive and regional development, growth, and differentiation of brain structures during the early foetal phase. The early foetal period was neither morphologically nor morphometrically uniform. The cerebral proportion (length/height) and the angle of cerebrum to the standard line at the lateral view of the cerebrum, which may reflect the growth and C-shape formation of the cerebrum, may be a candidate for subdividing the early foetal period. Future precise analyses must establish a staging system for the brain during the early foetal period. This study provides insights into brain structure, allowing for a correlation with functional maturation and facilitating the early detection of brain damage and abnormal development.
Kitazawa H, Fujii S, Ishiyama H, Matsubayashi J, Ishikawa A, Yamada S, Takakuwa T. Nascent nephrons during human embryonic development: Spatial distribution and relationship with urinary collecting system. J Anatomy 2021; 238, 455-466, in press.DOI: 10.1111/JOA.13308
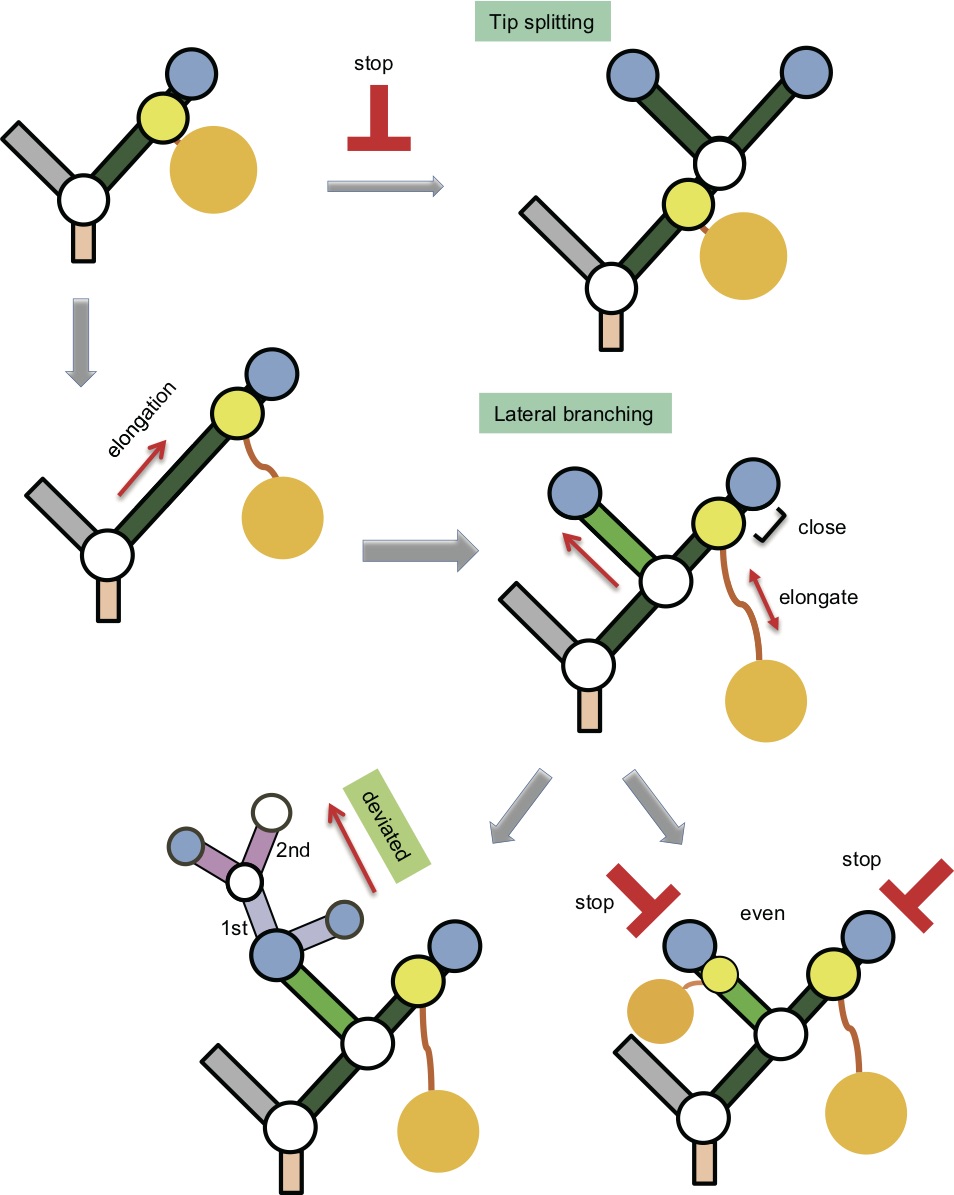
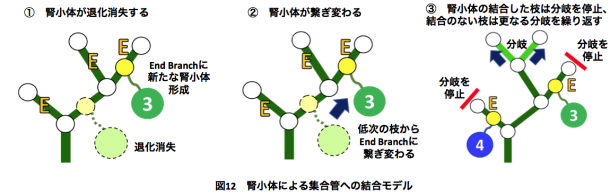
腎小体は尿路樹の末梢枝のみに結合するという観察を説明するモデル
Abstract
The two major components of the metanephros, the urinary collecting system (UCS) and nephron, have different developmental courses. Nephron numbers vary widely between species and individuals and are determined during fetal development. Furthermore, the development of nascent nephrons may contribute to the expansion of the proximal part of the UCS. This study investigated the distribution of nascent nephrons and their interrelationship with UCS branches during human embryogenesis. We obtained samples from 31 human embryos between Carnegie stages (CSs) 19 and 23 from the Kyoto Collection at the Congenital Anomaly Research Center of Kyoto University in Japan. Serial histological sections of the metanephros with the UCS were digitalized and computationally reconstructed for morphological and quantitative analyses. The three-dimensional (3D) coordinates for the positions of all UCS branch points, end points, attachment points to nascent nephrons (APs), and renal corpuscles (RCs) were recorded and related to the developmental phase. Phases were categorized from phase 1 to phase 5 according to the histological analysis. The UCS branching continued until RCs first appeared (at CS19). End branches with attached nascent nephrons (EB-AP[+]) were observed after CS19 during the fifth generation or higher during the embryonic period. The range of end branch and EB-AP(+) generation numbers was broad, and the number of RCs increased with the embryonic stage, reaching 273.8 ± 104.2 at CS23. The number of RCs connected to the UCS exceeded the number not connected to the UCS by CS23. The 3D reconstructions revealed RCs to be distributed around end branches, close to the surface of the metanephros. The RCs connected to the UCS were located away from the surface. The APs remained near the end point, whereas connecting ducts that become renal tubules were found to elongate with maturation of the RCs. Nascent nephrons in RC phases 3-5 were preferentially attached to the end branches at CS22 and CS23. The mean generation number of EB-AP(−) was higher than that of EB-AP(+) in 19 of 22 metanephros and was statistically significant for eight metanephros at CS22 and CS23. The ratio of the deviated branching pattern was almost constant (29%). The ratio of the even branching pattern with EB-AP(+) and EB-AP(+) to the total even branching pattern increased with CS (9.2% at CS21, 19.2% at CS22, and 45.4% at CS23). Our data suggest the following: EB-AP(+) may not branch further at the tip (i.e., by tip splitting), but branching beneath the AP (lateral branching) continues throughout the embryonic stages. Our study provides valuable data that can further the understanding of the interactions between the UCS and nascent nephrons during human embryogenesis.
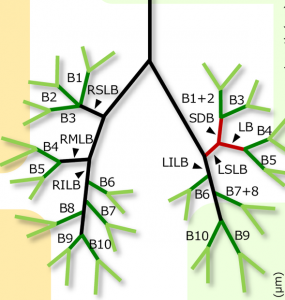
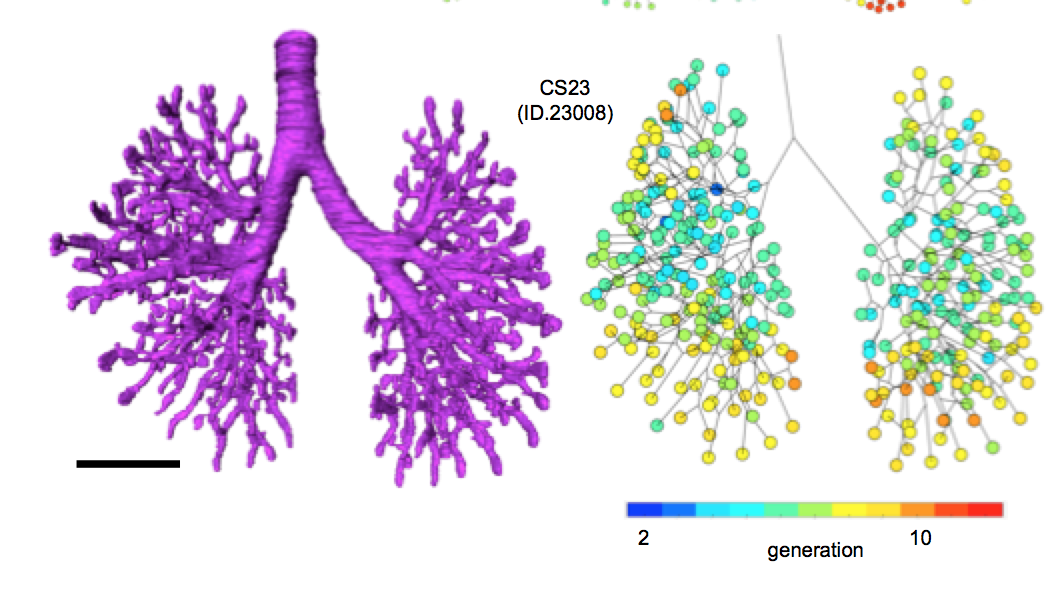
Fujii S, Muranaka T, Matsubayashi J, Yamada S, Yoneyama A, Takakuwa T. Bronchial tree of the human embryo: categorization of the branching mode as monopodial and dipodial, PLoS One 2021, Published: January 15, 2021, https://doi.org/10.1371/journal.pone.0245558
Abstract
Some human organs are composed of bifurcated structures. Two simple branching modes—monopodial and dipodial—have been proposed. With monopodial branching, child branches extend from the sidewall of the parent branch. With dipodial branching, the tip of the bronchus bifurcates. However, the branching modes of the human bronchial tree have not been elucidated precisely. A total of 48 samples between Carnegie stage (CS) 15 and CS23 belonging to the Kyoto Collection were used to acquire imaging data with phase-contrast X-ray computed tomography. Bronchial trees of all samples were three-dimensionally reconstructed from the image data. We analyzed the lobar bronchus, segmental bronchus, and subsegmental bronchus. After calculating each bronchus length, we categorized the branching mode of the analyzed bronchi based on whether the parent bronchus was divided after generation of the analyzed bronchi. All lobar bronchi were formed with monopodial branching. Twenty-five bifurcations were analyzed to categorize the branching mode of the segmental and subsegmental bronchi; 22 bifurcations were categorized as monopodial branching, two bifurcations were not categorized as any branching pattern, and the only lingular bronchus that bifurcated from the left superior lobar bronchus was categorized as dipodial branching. The left superior lobar bronchus did not shorten during the period from CS17 or CS18, when the child branch was generated, to CS23. All analyzed bronchi that could be categorized, except for one, were categorized as monopodial branching. The branching modes of the lobar bronchus and segmental bronchus were similar in the mouse lung and human lung; however, the modes of the subsegmental bronchi were different. Furthermore, remodeling, such as shrinkage of the bronchus, was not observed during the analysis period. Our three-dimensional reconstructions allowed precise calculation of the bronchus length, thereby improving the knowledge of branching morphogenesis in the human embryonic lung.
Ji X, Ishikawa A, Nagata A, Yamada S, Imai H, Matsuda T, Takakuwa T, Relationship between rectal abdominis muscle position and physiological umbilical herniation and return: a morphological and morphometric study. Anat Rec 2020, 303, 12, 3044-3051. doi: 10.1002/ar.24486
受諾は1年前だったのですが、ようやくpublishされました。
Abstract
The herniation of the intestinal loop (IL) in the extraembryonic coelom and its return to abdominal cavity is in parallel with the formation of the rectal abdominis muscle (RAM). Using high-resolution magnetic resonance imaging data of human fetuses (n = 19, CRL22-69 mm; stored at Kyoto Collection), this study aimed to analyze the relationship between the development of RAM and phase of IL herniation. The RAM runs at the lateral part of the abdominal wall in the small samples in the herniation phase. The position was shifted to the midline area in the larger samples in the herniation phase. According to fetal growth, the caudal ends of the muscles extended along the umbilical ring towards the pubis, though the caudal part of the RAMs were thin and faint in most of the samples. Length measurements related with the growth of the abdominal wall including RAM and abdominal circumference showed positive correlation with fetal growth. On the contrary, diastasis of RAMs and the width and area of the umbilical ring were almost constant according to fetal growth. Such morphometric value showed no obvious changes regardless of the phases of herniation. The ratio of the width and diastasis of the RAMs to the circumference was decreased, indicating that the closure of the ventral body wall was influenced by growth differences. The present data indicate that the formation of the abdominal wall including RAM is independent of the phase of IL herniation, whether in the extraembryonic coelom or in the abdominal cavity.
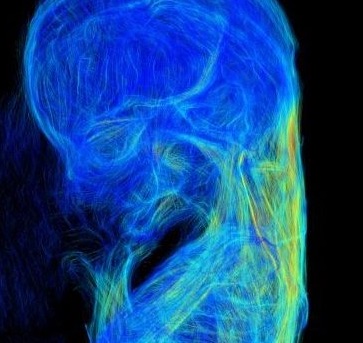
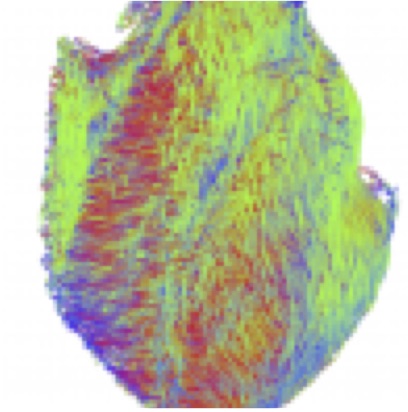
46. Nishitani S, Torii N, Imai H, Haraguchi R, Yamada S, Takakuwa T, Development of helical myofiber tracts in the human fetal heart: Analysis of myocardial fiber formation in the left ventricle from the late human embryonic period using diffusion tensor magnetic resonance imaging. Journal of the American Heart Association, 2020, 19(9) doi:10.1161/JAHA.120.016422
Abstract
Background
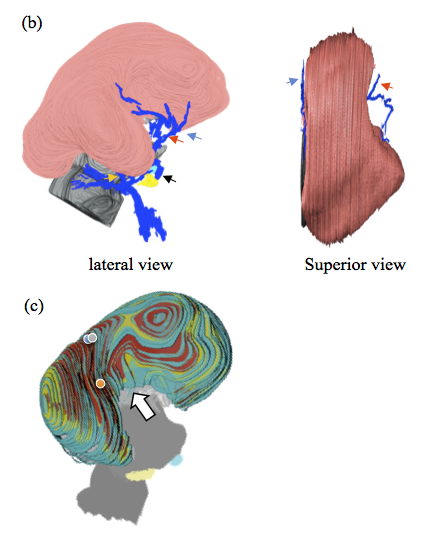
Detection of the fiber orientation pattern of the myocardium using diffusion tensor magnetic resonance imaging lags ≈12 weeks of gestational age (WGA) behind fetal myocardial remodeling with invasion by the developing coronary vasculature (8 WGA). We aimed to use diffusion tensor magnetic resonance imaging tractography to characterize the evolution of fiber architecture in the developing human heart from the later embryonic period.
Methods and Results
Twenty human specimens (8–24 WGA) from the Kyoto Collection of Human Embryos and Fetuses, including specimens from the embryonic period (Carnegie stages 20–23), were used. Diffusion tensor magnetic resonance imaging data were acquired with a 7T magnetic resonance system. Fractional anisotropy and helix angle were calculated using standard definitions. In all samples, the fibers ran helically in an organized pattern in both the left and right ventricles. A smooth transmural change in helix angle values (from positive to negative) was detected in all 16 directions of the ventricles. This feature was observed in almost all small (Carnegie stage 23) and large samples. A higher fractional anisotropy value was detected at the outer side of the anterior wall and septum at Carnegie stage 20 to 22, which spread around the ventricular wall at Carnegie stage 23 and in the early fetal samples (11–12 WGA). The fractional anisotropy value of the left ventricular walls decreased in samples with ≥13 WGA, which remained low (≈0.09) in larger samples.
Conclusions
From the human late embryonic period (from 8 WGA), the helix angle arrangement of the myocardium is comparable to that of the adult, indicating that the myocardial structure blueprint, organization, and integrity are already formed.
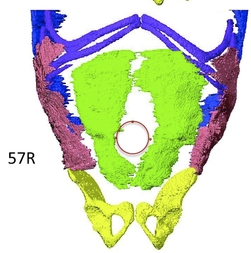
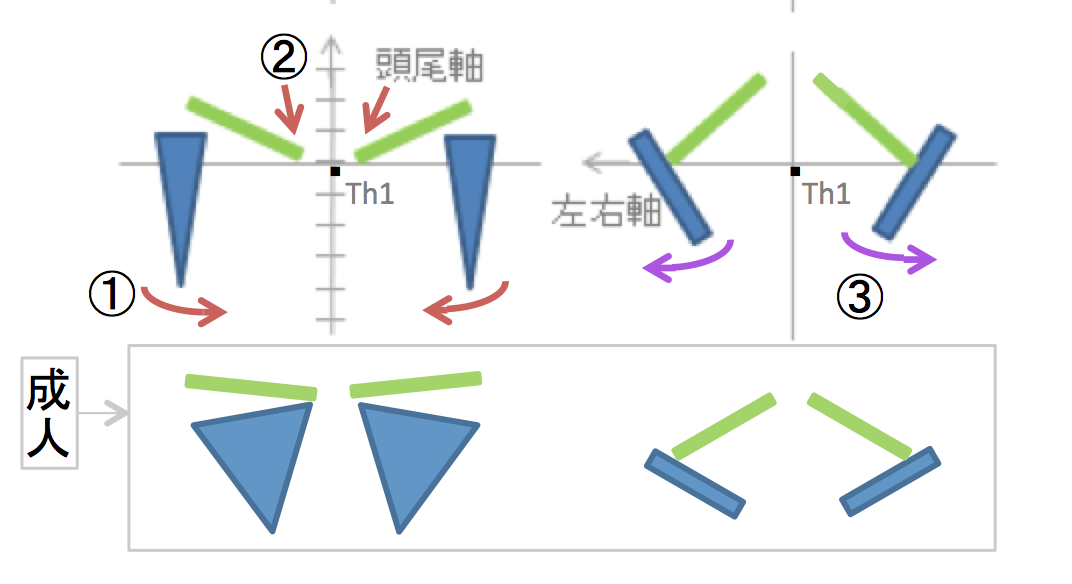
46. Tanaka S, Sakamoto R, Kanahashi T, Yamada S, Imai H, Yoneyama A, Takakuwa T. Shoulder girdle formation and positioning during embryonic and early fetal human development. PLoS ONE 2020, 15(9): e0238225. https://doi.org/10.1371/journal.pone.0238225
Abstract
Positional information on the shoulder girdle (the clavicle and scapula) is important for a better understanding of the function of the upper limb in the locomotive system as well as its associated disease pathogenesis. However, such data are limited except for information on the axial position of the scapula. Here, we describe a three-dimensional reconstruction of the shoulder girdle including the clavicle and scapula, and its relationship to different landmarks in the body. Thirty-six human fetal specimens (crown-rump length range: 7.6–225 mm) from the Kyoto Collection were used for this study. The morphogenesis and three-dimensional position of the shoulder girdle were analyzed with phase-contrast X-ray computed tomography and magnetic resonance imaging. We first detected the scapula body along with the coracoid and humeral head at Carnegie stage 18; however, the connection between the body and coracoid was not confirmed at this stage. During development, all landmarks on the shoulder girdle remained at the same axial position except for the inferior angle, which implies that the scapula enlarged in the caudal direction and reached the adult axial position in the fetal period. The scapula body was rotated internally and in the upward direction at the initiation of morphogenesis, but in the fetal period the scapula body was different than that in the adult position. The shoulder girdle was located at the ventral side of the vertebrae at the time of initial morphogenesis, but changed its position to the lateral side of the vertebrae in the late embryonic and fetal periods. Such a unique position of the shoulder girdle may contribute to the stage-specific posture of the upper limb. Adequate internal and upward rotation of the scapula could help in reducing the shoulder width, thereby facilitating childbirth. The data presented in this study can be used as normal morphometric references for shoulder girdle evaluations in the embryonic and fetal periods.
44. Fujii S, Muranaka T, Matsubayash J, Yamada S, Yoneyama A, Takakuwa T. The bronchial tree of the human embryo: an analysis of variations in the bronchial segments. J Anatomy 2020, 237, 311-322. doi: 10.1111/joa.13199.
Abstract
A classical study has revealed the general growth of the bronchial tree and its variations up to Carnegie stage (CS) 19. In the present study, we extended the morphological analysis CS by CS until the end of the embryonic period (CS23). A total of 48 samples between CS15 and CS23 belonging to the Kyoto Collection were used to acquire imaging data by performing phase-contrast X-ray computed tomography. Three-dimensionally reconstructed bronchial trees revealed the timeline of morphogenesis during the embryonic period. Structures of the trachea and lobar bronchus showed no individual difference during the analyzed stages. The right superior lobar bronchus was formed after the generation of both the right middle lobar bronchus and the left superior lobar bronchus. The speed of formation of the segmental bronchi, sub-segmental bronchi, and further generation seemed to vary among individual samples. The distribution of the end-branch generation among five lobes was significantly different. The median branching generation value in the right middle lobe was significantly low compared with that of the other four lobes, whereas that of the right inferior lobe was significantly larger than that of both the right and left superior lobes. Variations found between CS20 and CS23 were all described in the human adult lung, indicating that variation in the bronchial tree may well arise during the embryonic period and continue throughout life. The data provided may contribute to a better understanding of bronchial tree formation during the human embryonic period.